Maria Magdalena Gurzun1,2, Marinela Serban2, Ion Bostan2, Carmen Ginghina1,2, Bogdan A. Popescu1,2
1 University of Medicine and Pharmacy ”Carol Davila”, Euroecolab, Bucharest
2 Institute of Emergency for Cardiovascular Diseases ”Prof. Dr. C. C. Iliescu” Bucharest
Contact address:
Bogdan A. Popescu
University of Medicine and Pharmacy “Carol Davila”, Euroecolab,
Emergency Institute for Cadiovascular Diseases “Prof. Dr. C. C. Iliescu”
Sos.Fundeni 258, sector 2, 022328. Bucharest, Romania
Phone/Fax: +4021 3175227
e-mail: bogdan.a.popescu@gmail.com
A 78 year old man with a VVI pacemaker implanted in 2009 for sick sinus syndrome and lead replacement in 2012 for pacing dysfunction, was admitted for pocket infection and lead extravasation through the skin. The first lead was not removed at the time of second intervention in 2012 and the second implanted lead was a lead with active fixation. The chest X-ray (panel A) showed the two leads coming from the left subclavian vein through the right atrium into the right ventricle. The initial lead was adjacent to the right atrium lateral wall and was inserted in the right ventricle apex (white arrow) while the active fixation lead was adjacent to the interatrial septum and was inserted at the level of right ventricle anterior wall (yellow arrow). As one can notice on the chest X ray the lead protruding through the skin was the initially implanted one (white arrow), which was making a loop before the contact with the pacemaker (red asterisk) (panel A-C).
The transthoracic echocardiography showed the two leads in the right atrium (panel D). In the mid segment of one of them there was an echogenic and hypermobile structure highly suggestive of a vegetation (panel E). The 3D image of the right atrium (panel F) demonstrated that the structure was localized at the level of the lead located adjacent to the right atrium lateral wall (red arrow). Moreover, the transesophageal echocardiography confirmed that the structure was localized on the lateral lead (white arrow)(panel G). The 3D TEE imaging also showed clearly the structure highly suggestive of vegetation (panel H, red arrow). Therefore, the echocardiographic 2D and 3D visualization of the leads combined with the chest X-ray allowed the conclusion that the vegetation was localized on the first inserted lead.
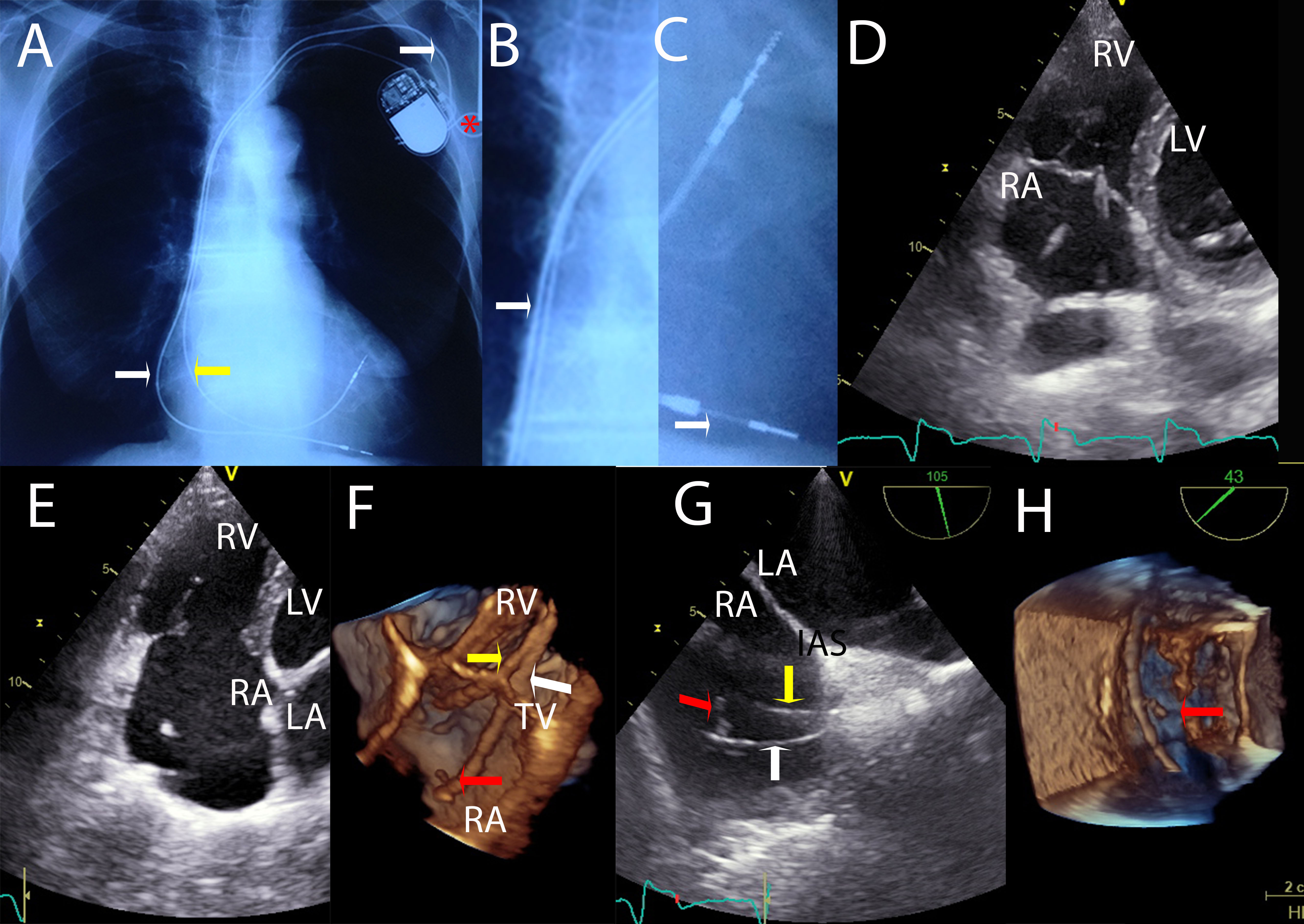
Figure 1. A The chest X-ray showed the two leads coming from the left subclavian vein through the right atrium into the right ventricle. A-C The chest X-ray the lead protruding through the skin was the initially implanted one (white arrow), which was making a loop before the contact with the pacemaker (red asterisk)
D The transthoracic echocardiography showed the two leads in the right atrium. E In the mid segment of one of them there was an echogenic and hypermobile structure highly suggestive of a vegetation. F The 3D image of the right atrium demonstrated that the structure was localized at the level of the lead located adjacent to the right atrium lateral wall (red arrow). G The transesophageal echocardiography confirmed that the structure was localized on the lateral lead (white arrow). H The 3D TEE imaging also showed clearly the structure highly suggestive of vegetation.
The echocardiographic appearance together with positive blood cultures indicated infective endocarditis of pacemaker lead. As the patient was not pacemaker dependent the leads were removed and the patient received antibiotic therapy with the indication of re-evaluation after 2 weeks.
Conflict of interest: none declared.
Abbreviations:
LA – left atrium;
LV – left ventricle;
RA – right atrium;
RV – right ventricle;
TV – tricuspid valve;
IAS – interatrial septum.
 This work is licensed under a
This work is licensed under a