Ileana Arsenescu
Article received on the 25th of November 2012. Article accepted on the 8th of February 2013.
“Prof. Dr. C. C. Iliescu” Emergency Institute of Cardiovascular Diseases, Bucharest, Romania
Arsenescu Ileana, MD, “Prof. Dr. C. C. Iliescu” Emergency Institute of Cardiovascular Diseases, 258 Fundeni Street, District no. 2, 022328, Bucharest, Romania.
56 years old hypertensive, dyslipidemic patient, with a personal history of smoking, known in the Cardiology clinic for recurring pectoral angina episodes. The patient presents bilateral latero-cervical murmurs and the systolic blood pressure measured on the left arm is 70 mm Hg higher than on the right arm.
Abreviations:
CCA common carotid artery
ICA internal carotid artery
ECA external carotid artery
SV systolic velocity
DV diastolic velocity
RI resistance index
Comments
Right side
– The inversed and internalized Doppler signal on the right ECA (Fig. 1 and Fig. 4) shows that the incomplete occlusion of the right CCA allows a blood supply to the ICA from the ECA, at the bifurcation
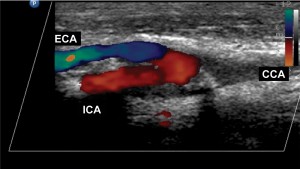
Figure 1. Right carotid axis. The CCA does not present color Doppler signal, except for the terminal portion, just before the bifurcation. The different color of the Doppler signal present in the ICA and ECA shows that the blood flows in opposite directions.
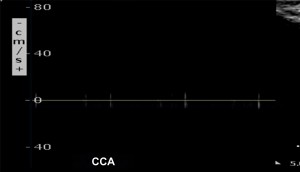
Figure 2. The proximal and medium portions of the right CCA do not register spectral Doppler signal.
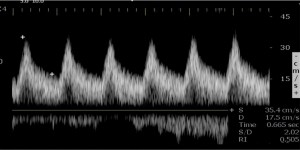
Figure 3. Right ICA: SV = 35 cm/s, DV 17 cm/s, RI = 0.50. The Doppler signal is anterograde. Low velocities, normal RI. A notable aspect is the slower systolic ascension.
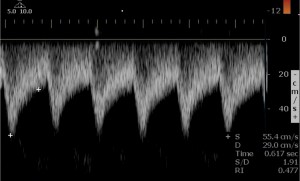
Figure 4. Right ECA: SV = – 55 cm/s, DV = – 29 cm/s, RI = 0.48. The Doppler signal is retrograde. We can notice the increased diastolic component and the very low resistance index.
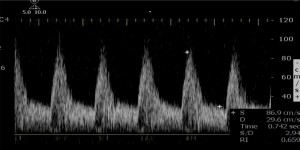
Figure 5. Right vertebral artery: SV = 67 cm/s, DV = 29 cm/s, RI = 0.66. Symmetrical increase of the systolic and diastolic velocities, with normal resistance index.
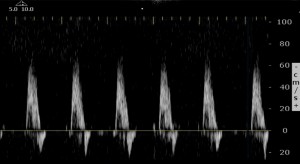
Figure 6. Right subclavian artery: SV = 65 cm/s. Without significant signal anomalies, except for the fading positive wave in the protodiastole, indicating low arterial elasticity.
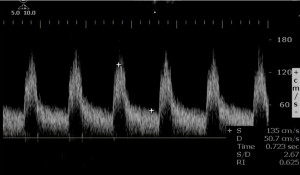
Figure 7. Left CCA: SV = 135 cm/s, DV = 50 cm/s, RI = 0.62). Slightly increased velocities. Normal resistance index.
– The right ECA has an incoming blood flow from the left ECA, where the Doppler signal has increased velocities and a degree of internalization suggested by the low resistance index (Fig. 9).
– The moderate increase of velocities on the left ICA (Fig. 8) show that it also has a role in compensating the occlusion of the right CCA, via the anterior communicating artery
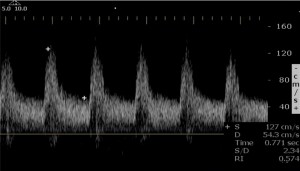
Figure 8. Left ICA: SV = 127 cm/s, DV = 54 cm/s, RI = 0.57. Slightly increased velocities. Normal resistance index.
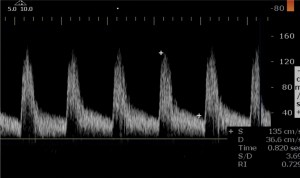
Figure 9. Left ECA: SV = 135 cm/s, DV = 36 cm/s, RI = 0.72. Slightly increased velocities. The resistance index is lower than 0.75, relatively low for an external carotid artery, suggesting a degree of flow internalization.
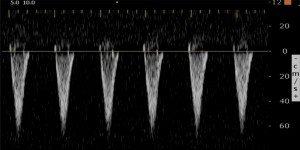
Figure 10. Left vertebral artery. The Doppler signal is totally reversed (5th grade arterial “blood theft”). The absence of the diastolic component suggests that the flow is directed to a high resistance territory.
Left side
– The hyperemic monophase Doppler wave, with a permanent anterograde diastolic component and the slow systolic ascension recorded in the subclavian artery (Fig. 11 and Fig. 12) is a typical, indirect sign found below a severe arterial lesion.
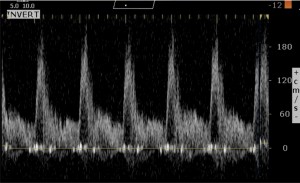
Figure 11. The left subclavian artery, in the sterno-clavicular region. Increased velocities and the turbulent flow show that the recording is made immediately after the occurrence of a severe lesion. The presence of a hyperemic monophase wave aspect with a significant diastolic component suggests that it is a severe lesion.
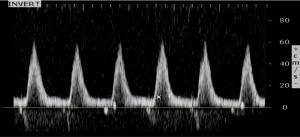
Figure 12. Left subclavian artery, after the emergence of the vertebral artery. The hyperemic monophase wave is maintained, with an increase in the systolic ascension time, an aspect typical for a poorly compensated, severe stenosis.
– The severity of the proximal subclavian artery lesion is confirmed by the complete flux inversion present in the vertebral artery (Fig. 10), now oxygenating the left superior limb. The Doppler curve lost its anterograde diastolic component, characteristic for a normal vertebral flux. Now it has the aspect of an artery supplying blood for a high resistance territory, like the left superior limb.
– The Doppler signal was normal on the right vertebral artery, thus eliminating the possibility of its involvement in compensating the occlusion of the right CCA, or in the “blood theft” phenomenon present in the left vertebral artery.
Conflict of interests: none declared.
 This work is licensed under a
This work is licensed under a