Roxana Oana Darabont
1 “Carol Davila” University of Medicine and Pharmacy, Department of Cardiology, Emergency University Hospital Bucharest
Contact address:
Roxana Oana Darabont, M.D., Ph.D.
Department of Cardiology, Emergency University Hospital Bucharest, 169 Splaiul Independentei, 050098 Bucharest, Romania. Fax: +40 21 3180576; Phone: + 40 723 441 315. E-mail: rdarabont@yahoo.com
A patient of 65 years old with end-stage renal disease has been referred by the nephrologist to our service of vascular ultrasound in order to be evaluated for a left brachiocephalic fistula realized one year ago. The hemodialysis becomes inefficient in the last two month.
The ultrasound examination was realized with an echograph Aloka Alpha 10 and a high-frequency linear array transducer.
We have applied a protocol for hemodialysis access evaluation, starting the interrogation at the level of the brachial artery supplying the fistula1. The volume flow of the fistula was measured with “flow profile” application and varied between 104-107 ml/min (Figure 1).
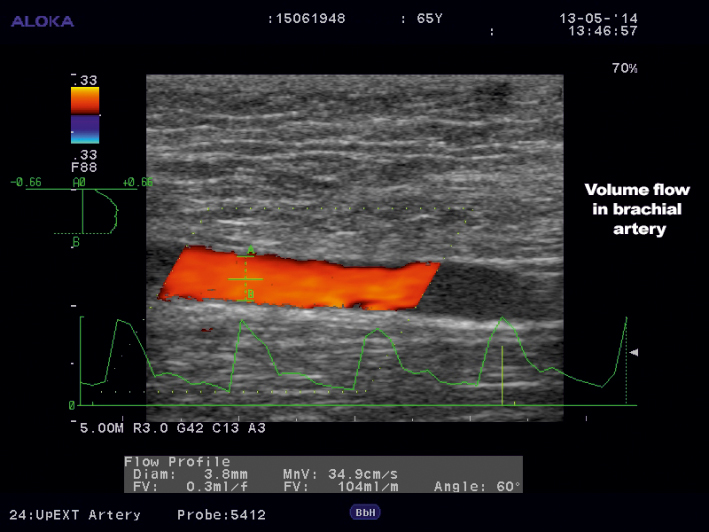
Figure 1. Duplex ultrasound imaging of the flow in the brachial artery supplying the hemodialysis fistula. Volume flow = 104 ml/min, at a beam angle = 60°.
This values have indicated a very decreased flow in the fistula. The usual measurements fall in the range 600-1500 ml/min. At a flow <300 ml/min it is signaled a high risk of thrombosis2. The volume flow is calculated by the formula:
Volume-flow (ml/min) = cross-sectional area (cm2) x mean velocity (cm/sec) x 60
The cross-sectional area can be obtained from the diameter of the artery and mean velocity from the weighted time-averaged velocity over a several cardiac cycles.
Next step of this ultrasound evaluation was to find out the reasons for which the flow was so low. Later complications of fistulas and grafts include: stenosis – usually in the vein, thrombosis, aneurysms/pseudoaneurysms and steal. The most common cause of low flow detection in native fistulas is stenosis, while in grafts is thrombosis2,3.
Flow in the supplying artery was of low-pulsatility pattern (Figure 2). Systolic velocities at the site of anastomosis were high – almost 300 cm/sec on the arterial side and on the venous side as well, difficult to be measured accurately (Figure 3 and 4). The cephalic vein was identified with two narrowed segments: one at 2 cm above the elbow joint, where peak systolic velocieties (PSV) of 471 cm/sec have been recorded (Figure 5) and a second one at 12 cm above elbow joint, with an incomplete thrombosis and a PSV of almost 60 cm/sec (Figure 6). Flow after the last stenosis had velocities of about 15 cm/sec (Figure 7).
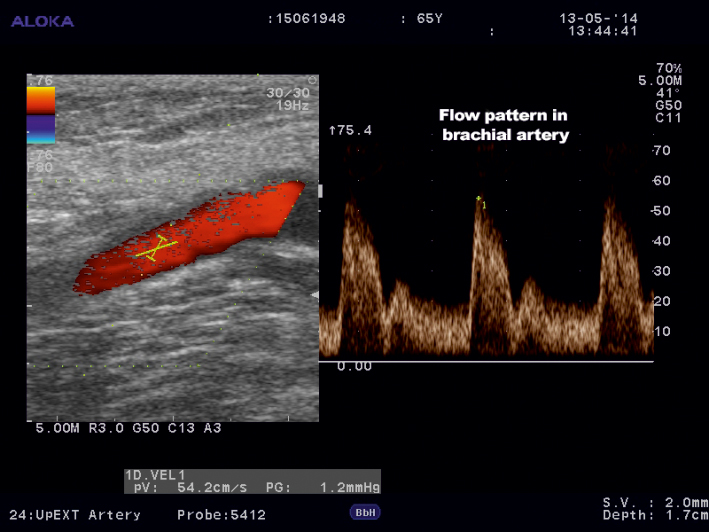
Figure 2. Color Doppler ultrasound of the brachial supplying artery indicating low-pulsatility pattern.
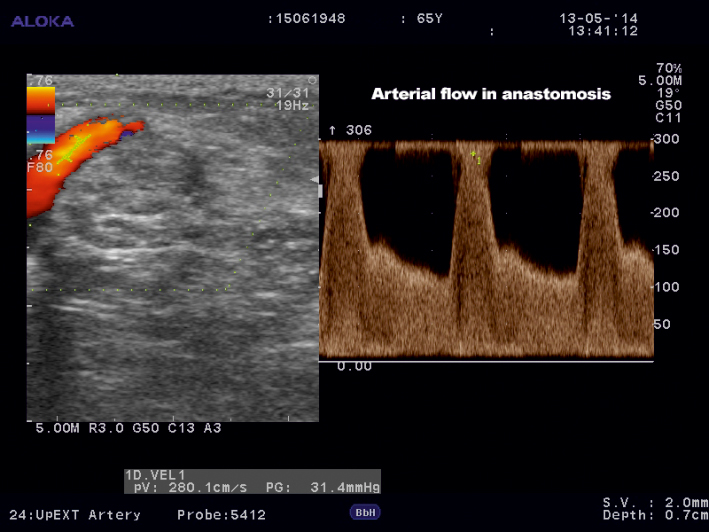
Figure 3. Color Doppler ultrasound of the brachial supplying artery at the level of anastomosis.
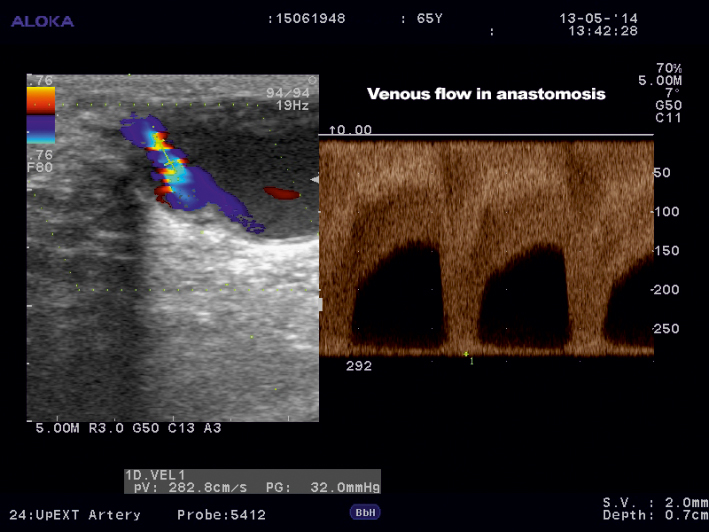
Figure 4. Color Doppler ultrasound of the cephalic vein at the level of anastomosis.
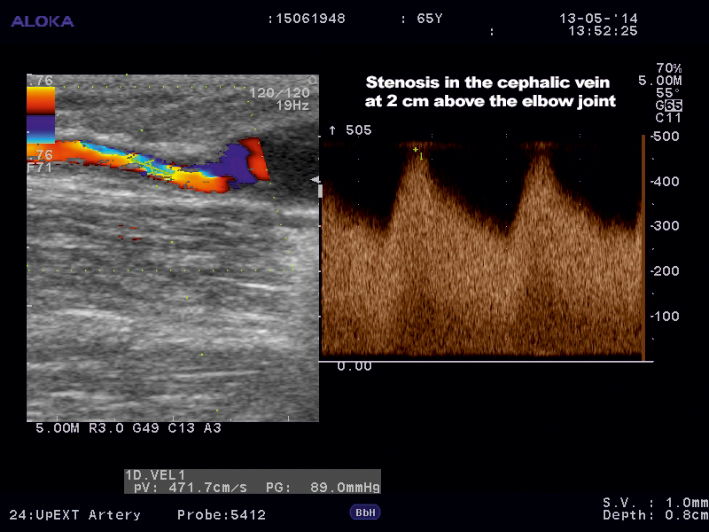
Figure 5. Color Doppler ultrasound of the cephalic vein. Stenosis at 2 cm above elbow joint.
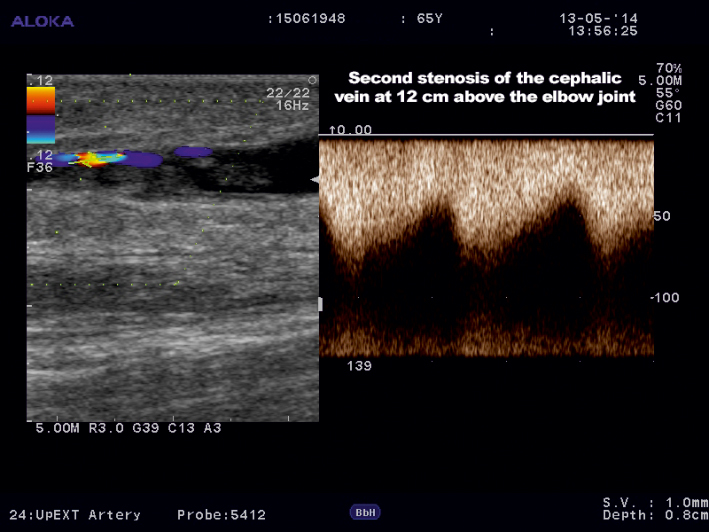
Figure 6. Color Doppler ultrasound of the cephalic vein. A second stenosis was identified at 12 cm above elbow joint.
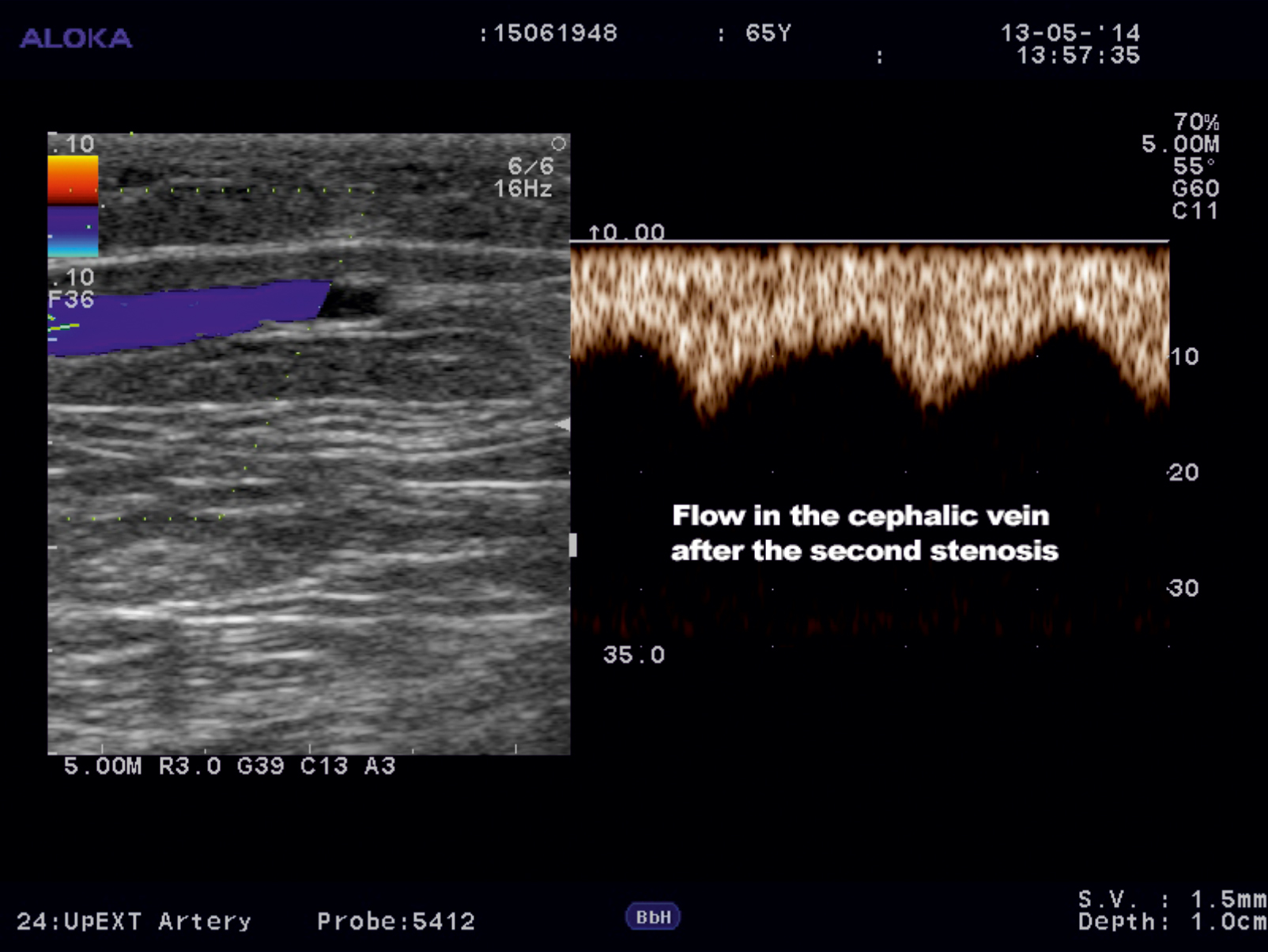
Figure 7. Color Doppler ultrasound of the cephalic vein after the second stenosis.
How can we interpret these hemodynamic findings? The flow in a functional fistula is characterized by very high velocities (200-300 cm/sec). The most recognized criteria to identify stenosis in the vessels supplying a fistula are PSV >400 cm/sec at the site of stenosis and/or PSV ratio of prestenotic or poststenotic flow to in-stenosis flow >3:14. In our case the velocities in the anastomosis could have a certain significance: the absolute value of PSV is not diagnostic for a significant stenosis (300 cm/sec), but the PSV ratio is (300/60=5). However, we consider that the stenosis that are compromising this vascular access are situated at the level of the cephalic vein: one revealed by PSV >400 cm/sec (471 cm/sec) and the other one by a PSV ratio of 4:1 (60/15).
In current practice color Doppler ultrasonography has replaced the angiography for the evaluation of hemodialysis access on the strength of important advantages: availability, non-invasivity and costs together with a high accuracy in diagnosis.
Conflict of interests: none declared.
Keywords: hemodialysis fistulas, complications of hemodialysis access, color Doppler ultrasound
References
1. ACCF/ACR/AIUM/ASE/IAC/SCA/SCVS/SIR/SVM/SVS/SVU 2013 appropriate use criteria for peripheral vascular ultrasound and physiological testing. Part II: Testing for venous disease and evaluation of hemodialysis access. Vasc. Med., 2013; 18:215-231
2. Colin D. – Ultrasound of hemodialysis access. In: “Vascular Ultrasound: Haw, Why and When”, Trush A., Hartshorne T. Eds, 3rd Ed., Churchill Livingstone Elsevier, 2010; 233-253
3. Visciano B, Riccio E, De Falco V, Musumeci A, Capuano I, Mmoli A et al. – Complications of native srteriovenous fistula: the role of color Doppler ultrasonography. Ther. Apher. Dial., 2014; 18:155-161
4. Older RA, Gizieski TA, Wilkowski MJ, NGLE JF, Cote DA – Hemodialysis access stenosis: early detection with color Doppler US, Radiology, 1998; 207:161-164
 This work is licensed under a
This work is licensed under a