Ioana Adriana Ghiorghiu, Mădălina Elena Iancu*, Marinela Şerban, Carmen Ginghină
”Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases, Bucharest
* “Regina Maria” Private Healthcare Network
Contact address:
Ioana Ghiorghiu, MD, “Prof Dr C.C. Iliescu” Institute of Emergency for Cardiovascular Diseases, Sos Fundeni No. 258, 022322, Bucharest.
E-mail: ioanagh2001@yahoo.com
Abstract: Premises – The elastic structure of the aorta permits it to act as a conduct for the cardiovascular system1. Its elastic properties moderate the left ventricle’s performance and help regulate the coronary flow. Patients undergoing aortic coarctation (AoCo) surgery suffer from a change in elasticity of the ascending aorta, favoring early atherosclerotic change2. This change of the vascular elasticity can be assessed using the elasticity indices: aortic strain, distensibility and stiffness. A change in the aortic elasticity parameters consequently determines hemodynamic changes, as well as alterations to the dimensions of the ascending aorta in patients who underwent AoCo corrective surgery. Materials and methods – 23 patients who underwent surgery for AoCo were included in the study, with a proper correction, supported by clinical and echocardiographic data. The control lot consisted of 20 healthy subjects. The two lots had a similar structure regarding age and sex. The vascular reactivity was assessed by aortic strain, distensibility and stiffness measured with TTE according to classic formulas. Results – Patients who underwent AoCo surgery presented modifications of the vascular reactivity indexes of the ascending aorta, respectively decreased distensibility capacity (p<0,001), reduced aortic strain (p<0,001), increased aortic stiffness (p<0,001) compared to the control lot. The dimensions of the ascending aorta are statistically significant greater, compared to a control lot consisting of healthy subjects. Conclusions – Assessment of vascular reactivity in the ascending aorta in patients who achieved correction of Ao Co shows a more rigid ascending aorta with diminished elasticity and distensibility, compared to a control group of healthy subjects. The elastic properties were highlighted by the assessment of classical vascular reactivity indices (stiffness, aortic strain and distensibility). The ascending aorta shows higher dimensions that are likely due to altered vascular reactivity at this level.
Keywords: Aortic coarctation, vascular reactivity, aortic strain, distensibility, stiffness, ascending aorta size
Rezumat: Premize – Artera aortă are o structură elastică care îi conferă o funcţie de conduct la nivelul aparatului cardiovascular1. Datorită proprietăţilor elastice contribuie la reglarea performanţei VS şi a fluxului coronarian. Pacienţii cu coarctaţie de aortă (Co Ao) operată prezintă o modificare a funcţiei elastice a aortei ascendente care predispune la modificări aterosclerotice precoce2. Această modificare a elasticităţii vasculare poate fi evaluată cu indicii de elasticitate: strain aortic, distensibilitate, rigiditate. Modificarea parametrilor de elasticitate aortici determină modificări ale hemodinamicii sanguine la acest nivel dar și ale dimensiunilor aortei ascendente la pacienţii post corecţia Co Ao. Material şi metodă – Au fost luați în studiu un număr de 23 pacienți cu coarctație de aortă operați cu datele clinice și ecocardiografice ale unei corecţii bine realizate și un lot control de 20 subiecţi sănătoşi, cele două loturi având o structură asemănătoare ca vârsta şi sex. Rezultate – Pacientii cu Co Ao operată au avut indici de reactivitate vasculară la nivelul aortei ascendente modificaţi, respectiv distensibilitate aortică redusă (p<0,001), strain-ul aortic redus (p<0,001), rigiditate aortică crescută (p<0,001) comparativ cu lotul martor. Dimensiunile aortei ascendente post corecţia Co Ao sunt semnificativ statistic mai mari comparativ cu un lot martor de subiecți sănătoşi. Concluzii – Evaluarea reactivităţii vasculare la nivelul aortei ascendente la pacienţii la care s-a realizat corecţia unei coarctaţii de aortă evidenţiază o aortă ascendentă mai rigidă, cu elasticitate şi distensibilitate diminuate. Aceste proprietăţi elastice au fost evidenţiate prin determinarea indicilor clasici de reactivitate vasculară (strain aortic, rigiditate şi distensibilitate). Aorta ascendentă prezintă dimensiuni crescute care sunt cu mare probabilitate determinate de reactivitatea vasculară modificată de la acest nivel.
Cuvinte cheie: Coarctaţie de aortă, reactivitate vasculară, strain aortic, distensibilitate, rigiditate, dimensiuni aortă ascendentă
Introduction
AoCo is a congenital heart disease benefiting from surgical correction since 19443 and interventional angioplasty since 19824. In this time frame, a large number of patients survived correction, representing a part of the “grown-up congenital heart disease” population. Studies conducted on these patients have revealed a wide spectrum of cardiovascular comorbidities, even in cases with a good anatomical result at the isthmic region.
Studies published in the literature have not succeeded in positively identifying the factors leading to post-correction complications. If the age of correction and a bicuspid aorta were documented by several studies6, the data for the other parameters (correction method, the remaining gradient in the itshmic region, the ankle-arm index) is contradictory. A new factor considered of great importance in the development of post-correction complications is currently investigated – the ascending aorta’s vascular reactivity.
Previous studies have shown an early vascular remodeling of the ascending aorta6 and of the vascular territory preceding the isthmic region. Vascular remodeling includes a modified vascular reactivity and an increase of intima media thickness at the level of the great arteries’8,9. The studies have revealed a more stiffer aorta, with a decreased elasticity, leading to aortic dilatation as the patient ages6,10. This modified vascular reactivity has been identified even in newly born babies and infants and it is detectable before the intervention and remains partially stable, even when the correction is succesfull11. The change in vascular reactivity seems to be the determining cause of post corrective surgery complications8,9,11,12. It has been proven that the changes of vascular reactivity leads to the increase of cardiovascular risk and early atherosclerosis. Identifying these problems at the level of the ascending aorta lead to a new vision of AoCo, which is no longer regarded as an isolated problem of the aortic isthm, but rather a generalized problem of the precoarctation vascular territory14.
Materials and methods
The study of vascular reactivity in the ascending aorta has been conducted on a lot consisting of 23 patients treated for AoCo (21 patients with surgical correction and 2 patients who underwent balloon angioplasty) (Table 1). They were admitted between 2001 and 2007 in ”Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases. The study also had a control lot of 20 healthy subjects with a similar distribution regarding sex and age to the ones present in the study lot.
Table 1. The characteristics of the study lot
| Patients (n=23) | Control lot (n=20) | p | |
| Age (years) | 28,65±9,98 | 29,70±10,92 | 0,789 |
| Sex (M/F) | 17/6 | 12/8 | 0,337 |
| Systolic BP (mmHg) | 123,04±13,63 | 114,50±13,56 | 0,034 |
| Diastolic BP (mmHg) | 75,22±11,63 | 73,00±10,81 | 0,300 |
| Corporeal surface (m²) | 1,81±0,21 | 1,79±0,21 | 0,826 |
Inclusion criteria:
- An interventional or surgical correction for AoCo
- Clinical criterion of a successful correction – normal pulse amplitude at the femoral arteries
- Echocardiographic criterion for a good correction – velocity in the ascending aorta <3 m/s and the absence of anterograde diastolic flux (diastolic tail)
- Normal blood pressure values with/without antihypertensive drugs
Exclusion criteria:
- Significant aortic insufficiency (>IIIrd degree according to the echocardiographic classification
- Aortic stenosis
- Aortic metallic prosthesis
- Arterial hypertension (patients without treatment or with uncontrolled values under treatment)
- Significant stenosis (post-corrective gradient >30 mmHg)
The patients were excluded because we considered that they present lesions accompanied by significant hemodynamic alterations, influencing the vascular elasticity parameters calculated for the ascending aorta.
Analyzing the male/female ratio we notice a slight preponderance of the male patients. The BP values were significantly higher in patients who underwent corrective surgery for AoCo, compared to healthy subjects (p<0.05 but were within normal limits for all the patients enrolled in the study).
The parameters parameters for vascular reactivity of the ascending aorta:
The following classic aortic elasticity indices were measured15:
- Aortic strain = 100 (Ao S – Ao D)/Ao D
- Aortic distensibility index = (2(Ao S – Ao D)/Ao D(PP)) (10-6cm2dyne-1)
- Aortic stiffness index (SI) = ln (SBP/DBP)/ ((Aos – AoD)/AoD)
The dimensions of the aorta were: AoS – systolic diameter, AoD – diastolic diameter (as measured in 2D guided M mode, 3 cm above the aortic valve, Ao D measured at the peak of the R wave, with a simultaneous EKG, Ao S measured at the maximum anterior movement of the aortic wall) (Figure 1). The values of the blood pressure are represented by SBP = Sistolic blood pressure, DBP = diastolic blood pressure – values measured at the right arm.
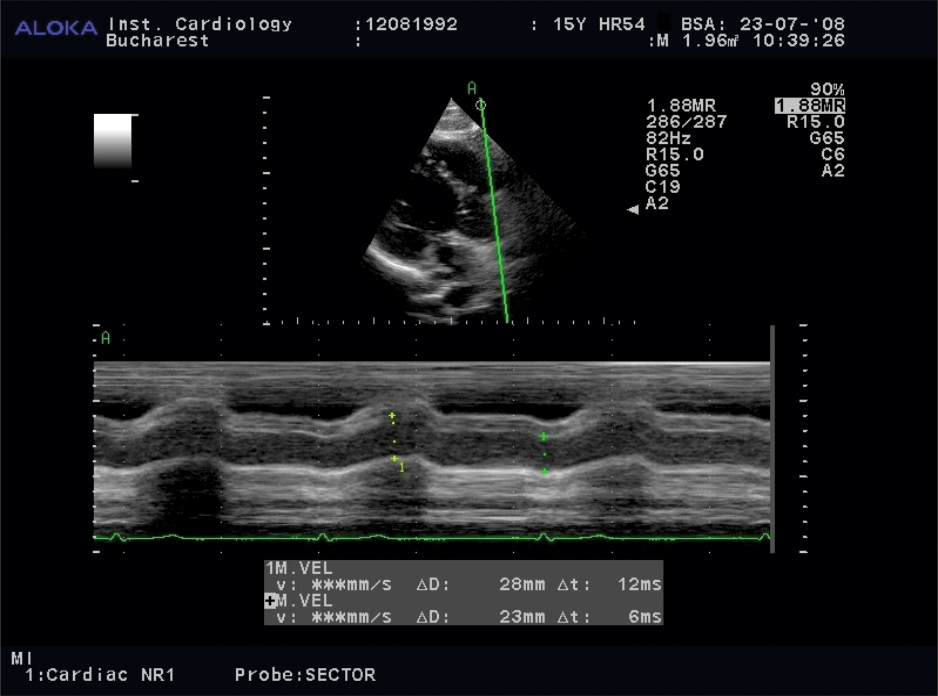
Figure 1. Measuring the aortic dimensions in 2D guided M mode, in order to calculate the elasticity parameters of the ascending aorta. The M mode section is perpendicular to the long axis of the ascending aorta. The AoS and
the AoD are measured.
There are few papers in the literature studying the elastic function of the aorta post AoCo corrective surgery, using these parameters7,11,14.
The echocardiographic examination was performed with an Aloka Alpha 10 Prosound (Aloka Japan) device. The echocardiographic images were recorded simultaneously with an EKG signal, with at least 3 sinus rhythm cardiac cycles being recorded, using the median value of the measurements. The patients were examined in left lateral decubitus postion, with a 4MHz transducer.
The aortic elasticity parameters were determined by using an echocardiography transducer set for M mode examination guided by a 2D image (we considered it necessary to place the M mode perpendicularly on the long axis of the ascending aorta in order to measure the maximal diameters)14. The patient was placed in left lateral decubitus and a long parasternal axis section was performed. The following parameters were measured in M mode section, placed 3 cm above the aortic ring, using the “edge to edge” technique:
- AoS – the systolic diameter of the ascending aorta – it is measured at the point of the maximum anterior movement of the aortic wall
- AoD – the diastolic diameter of the ascending aorta – it is measured at the end of the diastole, corresponding to the Q wave on the EKG
The dimensions of the ascending aorta and of the aortic arch were measured from the suprasternal view, also from this view were measured the dimensions of the great vessels. The dimension of the abdominal aorta was measured from the subcostal view. Blood pressure was measured on the right arm, immediately after the beginning of the echocardiographic examination. An aneroid capsule sphygmomanometer was used, with an adequately sized cuff for the arm’s width (the width of the cuff >2/3 of the diameter of the arm). The auscultation method was employed.
The statistic analysis of the data was performed by using SPSS software, v. 14.0 for Windows. The data was presented in percentiles and as median values ± standard deviation (SD) for the continuous variables. The differences between the different group’s median values were compared by using the t test for independent variables, the Mann – Whitney U, or Wilcoxon test. A p <0.05 was considered to be statistically significant and a p<0.01 was considered highly significant.
Results
Different measurements of the aorta were performed at various levels, as well as measurements of the origins of the large vessels emerging from the ascending aorta:
- The aortic ring
- The aorta at the level of the Valsalva sinuses
- The ascending aorta 3 cm from the aortic ring, in a parasternal long axis
- The aortic cross (before the origin of the left common carotid artery)
- The descending aorta, below the isthmic region
- The abdominal aorta
- The origin of the left common carotid artery
- The origin of the left subclavian artery
The values obtained through 2D measurements were considered in relation to the corporeal surface. The median values obtained were indexed with the corporeal surface and are presented in Table 2, compared to the values recorded for the control lot:
The dimensions of the aorta were significantly higher at the level of the aortic ring (11+/-1,5 mm/m2 versus 9,9 +/- 0,8 mm/m2), the ascending aorta (3 cm above the aortic ring), (17,3 +/- 5,6 mm/m2 versus 13,4 +/- 1,8 mm/m2) and abdominal aorta(9±1,99 mm/m2 versus 7,24±1,34 mm/m2) in patients suffering from AoCo, compared to the healthy subjects. The dimensions measured at the level of the Valsalva sinuses were also higher, but the p value was not statistically significant.
The values obtained for the aortic cross in patients who underwent surgery were smaller than the ones obtained for the control lot, but without any statistic significance. Higher values (statistically significant) were obtained at the origin of the great vessels (left subclavian artery, left common carotid artery), starting from the aortic cross in patients with surgically corrected AoCo, compared to the control lot.
Table 2. The dimensions of the aorta and of the great vessels originating from the aorta
| Aortic artery diameters indexed with the corporeal surface | Patients operated for AoCo | Control lot | p |
| Aortic ring (mm/m²) | 11±1,5 | 9,9±0,8 | 0,004 |
| Aorta – Valsalva sinuses (mm/m²) | 18,5±5,8 | 15±1,8 | 0,01 |
| Ascending aorta (mm/m²) | 17,3±5,6 | 13,4±1,8 | 0,003 |
| Aortic cross | 10,73±2,19 | 11,38±1,94 | 0,400 |
| Left common carotid artery – origin (mm/m²) | 3,46±0,67 | 2,94±0,35 | 0,003 |
| Left subclavian artery – origin (mm/m²) | 5,27±1,35 | 4,78±1,02 | 0,005 |
| Descending aorta (mm/m²) | 9,00±2,06 | 8,02±1,29 | 0,100 |
| Abdominal aorta (mm/m²) | 9,00±1,99 | 7,24±1,34 | 0,002 |
| p <0.01 statistically significant p <0.005 highly statistically significant |
|||
The elasticity indices of the ascending aorta for patients operated for AoCo were compared to elasticity indices obtained from the ascending aorta of healthy subjects. The results are presented in Table 3.
Table 3. Vascular reactivity indices
| Patients | Control lot | p | |
| Aortic distensibility (10-6 cm²dyne-1) (Ao dis) |
3,97±2,44 | 11,44±5,97 | <0,001 |
| Ao strain (%) | 9,17±6,20 | 23,85±11,16 | <0,001 |
| Aortic stiffness (aortic stiffness) (AoSI) |
10,17±6,17 | 2,19±0,89 | <0,001 |
The distensibility and aortic strain indices are statistically significant lower in the ascending aorta and stiffness indices are statistically significant higher in patients, compared to the control lot, contouring the picture of a less elastic, less distenssible, but stiffer ascending aorta.
The correlation between the dimensions of the ascending aorta and aortic elasticity indices
A correlation between the dimensions of the aorta measured as previously mentioned and the vascular reactivity indices (calculated by using unanimously accepted formulas – distensibility, aortic strain and aortic stiffness) was done in order to obtain an objective view of the influence of the modified aortic vascular reactivity on the dimensions of the ascending artery. The results are presented in Table 4.
Table 4. The correlation between the dimensions of the ascending aorta and aortic elasticity indices
| Aortic distensibility | Aortic strain | Aortic stiffness | |
| Aorta – ring | -,492(**) | -,477(**) | ,630(**) |
| Aorta – Valsalva sinuses | -,607(**) | -,585(**) | ,704(**) |
| Ascending aorta | -,595(**) | -,565(**) | ,700(**) |
| Aortic cross | -0,14 | -0,11 | 0,13 |
| Left common carotid artery – origin (mm/m²) | -,402(**) | -,427(**) | ,408(**) |
| Left subclavian artery – origin (mm/m²) | -0,23 | -0,2 | 0,21 |
| Descending aorta (mm/m²) | -0,24 | -0,24 | 0,24 |
| Abdominal aorta (mm/m²) | -0,23 | -0,21 | 0,29 |
| *p <0.05 – statistically significant **p <0.001 – highly statistically significant |
|||
The dimensions of the aorta at level of the aortic ring, Valsalva sinuses and ascending aorta negatively correlate with aortic distensibility and aortic strain (a less distensible aorta is larger at the level of the aortic ring), but is positively correlated to the aortic stiffness (a more rigid aorta has greater dimensions measured at the aortic ring). All 3 correlations have p <0.001. A negative correlation is suggested between the dimensions of the aorta at the aortic cross and distensibility and aortic strain. A positive correlation is suggested between the afore mentioned dimensions and the aortic stiffness, both without statistically significant indices. The aortic cross was the only segment of the aorta which had smaller dimensions in patients who underwent corrective surgery for AoCo, compared to the central lot, revealing once more a degree of hypoplasia of the aortic cross in these patients. The left common carotid artery negatively correlates with the distensibility and aortic strain indices and a positive correlation with the aortic stiffness index, with p <0.001. We can conclude that the less distensible, more stiffer aortic pattern is maintained in the left common carotid artery. The same types of correlations are present in the descending and abdominal aorta, as well as in the left subclavian artery, without statistically significant p values. Moreover, for these last results, it is important to mention and discuss the fact that the thoracic descending aorta and the abdominal aorta represent the aortic territory situated below the coarctation, with a different vascular reactivity. The left subclavian artery has its own particularity, as the main source for collateral circulation. Its dilatation is owed mostly to the increased preoperatory debit and less to the vascular reactivity changes.
Discussions
Previous studies published in the literature have shown the presence of an early vascular remodeling in the ascending aorta7,11,14 and in the precoarctation vascular territory. Vascular remodeling includes an altered vascular reactivity and the increase of the intima media thickness of the endovascular layer of the large vessels8,9. Studies revealed a more stiffer aorta, with decreased elasticity, resulting in a tendency to dilate in time10,11. This modified vascular reactivity was identified beginning with infants7, it is present before the correction and remains partially unmodified even when the corrective surgery was successful11. The changes in vascular reactivity seem to be the determining cause of most postsurgery complications8,9,11,12.
Vascular reactivity indices have presented the following particularities in patients who underwent corrective surgery for AoCo:
- Distensibility (3,97±2,44 10-6cm2dyne-1 in patients with AoCo versus 11,44 ± 5,72 10-6cm2dyne-1 in healthy subjects) and aortic strain (9,17±6,2% in patients with AoCo versus 23,85±11,16% in healthy subjects) registered lower values than normal, thus the capacity of the ascending aorta to expand itself and store kinetic energy at the moment of impact with the blood pumped by the heart during the systole is low.
- Aortic stiffness registered increased values (10,17 ± 6,17 in patients with AoCo versus 2,19 ± 0,89 in healthy subjects), characterizing a more stiffer aorta, probably secondary to the particular anatomical structure.
The results of this study show that the vascular reactivity indices characterizing the elastic nature of the ascending aorta are modified even in cases with a good correction of the isthmic lesion. The modifications in the elastic properties of the ascending aorta change the hemodynamic behavior at this level and influences BP, velocity and the irrigation pattern of two very important arterial territories: the carotid and the coronary systems. The modified elasticity parameters in the ascending aorta determine an increase of the vascular resistance in the precoarctational territory. We can conclude that the after load of the LV, which is much higher before the correction, decreases – but does not return to normal values after corrective surgery. This might be one of the factors determining the persistence of increased BP values, despite a good anatomical result after the correction of an AoCo8.
Considering the vascular reactivity of the arterial system in patients with corrected AoCo it seems to be divided in two segments with particular reactivity: the more rigid, less elastic precoarctation segment and the post coarctational segment, with a normal vascular reactivity. The two segments react differently during an effort, determining a dynamic tightening of the isthmic region, even in cases with a good anatomical correction11. This could partially explain the persistence of high BP values after corrective surgery, especially during an effort. On the other hand, constantly increased blood pressure values can determine the fragmentation of the elastin fibers from the media layer and changes in the intima layer, determining early atherosclerotic lesions. Hence, increased blood pressure values can be both cause and effect of the modified vascular reactivity.
The modified vascular reactivity has long term consequences on the function of the LV (both the systolic and diastolic components)13 and on the irrigation of the myocardium via the coronary arteries. These consequences appear as a result of the modification induced in the blood velocity and in the behavior of the reflected wave. The residual hypertrophy of the LV walls can be partially explained by the increased stiffness and decreased distensibility12.
Histology studies conducted on aortic tissue samples obtained from the AoCo resection area have revealed a larger quantity of collagen and a smaller quantity of smooth muscle fibers in the precoarctation area of the aorta, than in the area located below the coarctation16. These histological modifications are the basis of the functional changes previously described and have led to the conclusion that this arterial malformation is a generalized arteriopathy of the precoarctational area and not just an anomaly located in the isthmic region. This global approach of the precoarctational arterial system could better explain the complications connected to the arterial wall (aneurysms, early atherosclerotic lesions, aortic dissection) and the early age of debut, compared to the general population.
The median age of the patients in the lot for which vascular reactivity was studied was 28.65±9.98 years. This is an age characterizing a young population, but with a series of complications connected to the arterial wall, associating increased intima median thickness of the carotid, a subclinic marker of atherosclerotic lesions. The median age for the diagnosis of vascular reactivity changes raises the valid question of what is the age for the onset of these reactivity modifications. There are studies conducted on lots of newly-born babies and infants, suffering from AoCo, pre and post operatory7, which have demonstrated that even infants have preoperatory changes of the vascular reactivity. These modifications persist in the postoperative period. The described modifications are similar to those described by the present study, respectively reduced elasticity, reduced distensibility and an increased stiffness.
Considering the fact that these parameters can be measured with an echocardiograph which does not require supplementary programs and the validation through various studies of these indices obtained by transthoracic echocardiogram (non-invasive method) we can ask ourselves as cardiologists whether or not these indices could be determined in series for these patients, in order to quantify the risk of complications connected to the arterial wall. The vascular reactivity indices (distensibility, strain and stiffness) proved to be useful in long term care of patients suffering from Marfan syndrome, with a greater capacity of prediction regarding the risk of dissection and aortic rupture than the dimensions of the aorta13. In patients suffering from Marfan syndrome it has been demonstrated that aortic dissection can appear even in patients who do not present a significant dilatation of the ascending aorta, but have altered vascular reactivity indices.
The dimensions of the ascending aorta
Altered elasticity properties of the ascending aorta modify not only the hemodynamic behavior at this level, but also the dimensions of the ascending aorta11,14,17.
In patients suffering from AoCo the aorta is more dilated at the aortic ring (11±1.5 mm/m2 corporeal surface for patients versus 9.4±0.8 mm/m2 corporeal surface for healthy subjects), Valsalva sinuses (18,5±5,8 mm/m² corporeal surface for patients versus 15±1,8 mm/m2 corporeal surface for healthy subjects) and ascending aorta 17,3±5,6 mm/m2 corporeal surface for patients versus 13,4±1,8 mm/m2 corporeal surface for healthy subjects). These increased dimensions can be the consequence of modifications in the media layer, which has a small number of smooth muscle fibers and a larger number of collagen fibers which suffer a degradation process over time, leading to a progressive dilatation at this level11. This takes us to the conclusion that the aortic dilatation present at the aortic ring and ascending aorta are secondary to the particular histological structure of the ascending aorta and not a consequence of the associated aortic valve lesions.
The histological basis of the anatomic modifications is represented by a particular structure of the ascending aorta, especially in the aortic media layer, which contains elastic fibers with a particular structure, with a reduced capacity of elastic recoil at the moment of impact with the blood, permitting a gradual plastic deformation of the ascending aorta17. The same type of histological structures of the ascending aorta is described in several afflictions: Marfan syndrome, bicuspid aortic valve, aortic coarctation). There are no histological and genetic comparative studies for these diseases. Such studies could have revealed whether or not the microscopic anatomic structure is identical and if the determining genetic modification is similar. However, several studies have succeeded in creating an objective view of the functional behavior of the ascending aorta, which is similar in all of these patients7,11.
This study has identified statistically significant modifications in the size of the left common carotid artery (3.46±0.67 mm/m2 corporeal surface for patients versus 2.94±0.35 mm/m2 corporeal surface for healthy subjects) and left subclavian artery (5.27±1.35 mm/m2 corporeal surface for patients versus 4.28±1.02 mm/m2 corporeal surface for healthy subjects). In the case of the left subclavian artery the dilatation at the point of origin can be explained by the fact that it is the source of the collateral circulation and its dilatation is a characteristic of AoCo. However, the persistence of this dilatation after the correction of the lesion can only be partially explained in this manner. This dilatation is most likely owed to the particular anatomical structure of the precoarctational arteries. The origin of the left common carotid artery is more dilated in patients than in the control lot, further supporting the idea that the precoarctational arteries have a particular anatomical structure, favoring a progressive dilatation of the vessel at this level, despite a successful correction.
Conclusions
The evaluation of the elastic properties of the ascending aorta has shown a more stiffer (aortic stiffer in patients 10.17±6.17 versus 2.19±0.89 in healthy subjects, p <0.001), less distensible (distensibility in patients 3.97±2.44 10-6 cm2dyne-1 versus 11.44±5.92 10-6 cm2dyne-1 in healthy subjects, p <0,001) aorta, with a diminished elasticity (aortic strain in patients 9.17±6.20% versus 23.85±11.16% in healthy subjects, p <0.001) after the correction of the AoCo.
An increase in the dimensions of the ascending aorta appears secondary to the changes in the vascular reactivity.
The evaluation of the ascending aorta’s elastic properties by the determination of vascular reactivity represents the transition to the direct functional evaluation of the ascending aorta.
By determining both the dimensions of the ascending aorta, as well as the vascular reactivity indices, this study represents a complex evaluation, both morphological, as well as functional of the ascending aorta in patients who have previously underwent corrective surgery for an isthmic AoCo.
Conflict of interest: none declared.
Bibliography
1. O´Rourke MF, Hashimoto J – Mechanical factors în arterial aging. A clinical perspective, Journal of American College of Cardiology 2007; 50;1-13
2. Soon Yong Suh, Eung Ju Kim, Cheol Ung Choi et col– Aortic Upper Wall Tissue Doppler Image Velocity: Relation to Aortic Elasticity and Left Ventricular Diastolic Function, Echocardiography: A Journal of Cardiovascular Ultrasound@ Allied Tech,vol 26, issue 9, october2009, pg 1064-1074
3. Kaemmerer Harald în Gatzoulis MA, Webb DG, Daubeney Piers EF – Diagnosis and Management of Adult Congenital Heart Disease, Ed Churchill Livingstone, 2004, pg 253-265
4. Morriss Mary HJ, Mc Namara Dan G în Garson Arthur Jr, Bricker Timothy J, Fisher David J, Neish Steven R- The Science and Practice of Pediatric Cardiology, second edition, Ed Williams and Wilkins, 1998, pg 1317-1346
5. Eric Rosenthal: Coarctation of the aorta from fetus to adult:curable condition or life long disease process?;Heart 2005;91:1495-1502
6. Yskert von Kodolitsch, Muhammet A Aydin, Dietmar H Koschyk et col– Predictors of Aneurysmal Formation After Surgical Correction of Aortic Coarctation, Journal of the American College of Cardiology, 2002, 39,no4, 617-623
7. Vogt M, Kühn A, Baumgartner D et col– Impaired Elastic Properties of teh Ascending Aorta în Newborns, Before and Early After Successful Coarctation Repair – Proof of a Systemic Vascular Disease of the Prestenotic Arteries, Circulation, 2005;111;3269-3273
8. de Divitiis M, Pilla C, Kattenhorn M et col– Ambulatory Blood Pressure, Left Ventricular Mass and Coduit Artery Function Late After Successful Repair of Coarctation of the Aorta, Journal of the American College of Cardiology, 2003, vol 41, 12, 2259-2265
9. Meyer AA., Joharchi MS, Kundt G, Schuff – Werner P, Steinhoff G, Kienast W – Predicting the risk of early atherosclerotic disease development în children after repair of aortic coarctation, European Heart Journal, (2005), 26, 617-622
10. Iancu M E, Ghiorghiu I, Serban M, Craciunescu I, Hodo A, Popescu BA Ginghina C – Determinants and pattern of ascending aorta dilatation in patients with repaired aortic coarctation, European Journal of Echocardiography(2010)11(suppl2/ii58-ii86 doi)
11. Vitarelli A, Conde Y, Cimino E et col– Assessment of Ascending Aorta Distensibility After Successful Coarctation Repair by Strain Doppler Journal of American Society of Echocardiography 2008 Jun; 21(6):729-36.
12. Yat Yin Lam, Mullen JM, Kaya M, Wei Li, Gatzoulis MA, Henein MY – Left ventricular long axis dysfunction în adults with corrected aortic coarctation is related to an older age at intervention and increased aortic stiffness, Heart 2009 May;95(9):733-9
13. de Groot E, Hovingh GK, Wiegman A, et al Measurement of arterial wall thickness as a surrogate marker for atherosclerosis. Circulation 2004;109;Suppll1;III 33-8
14. Nistri S, Grande Allen J, Noale M et col– Aortic elasticity and size în bicuspid aortic valve syndrome, European Heart Journal, doi 10.1093; eurheartj/ehm 528, 20 dec 2007
15. Nichols W Wilmer – Clinical Measurement of Arterial Stiffness Obtained From Non Invasive Pressure Wave Forms, American Journal of Hypertension, 2004, 10.009 doi 10.1016
16. Sehested J, Baandrup U, Mikkelsen E, Different reactivity and structure of the prestenotic and post stenotic aorta în human coarctation: implication for baroreceptor function.Circulation, 1982;6;1060-1065
17. Nistri S, Sorbo MD, Marin M et al, Aortic root dilatation in young man with normally functioning bicuspid aortic valves Heart 1999;82; 19-22
 This work is licensed under a
This work is licensed under a