Valentin Chioncel1,2, Anamaria Avram1,2, Alexandru Cristian Ion1,2, Crina Sinescu1,2
1 “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
2 Bagdasar Arseni Emergency Hospital, Department of Cardiology, Bucharest, Romania
Abstract: De Winter T waves are a rare presentation for patients with acute LAD occlusion, some authors considering this pattern to be an equivalent of anterior ST elevation myocardial infarction (STEMI)1. We present the case of a 41 years old male presenting with a 3 hours continuous chest pain. The ECG pattern revealed the De Winter pattern with upsloping ST depression (>1 mm at J-point) in the precordial leads V3-V4 and peaked anterior T waves, with the ascending limb of the T wave commencing below the isoelectric baseline. The biochemical markers of myocardial necrosis were positive. Transthoracic echocardiography (TTE) revealed akinetic interventricular septum (IVS), apex and apical inferior wall with mild-moderate systolic left ventricle (LV) dysfunction. After receiving the guideline recommended antiplatelet and anticoagulant therapy (600mg Clopidogrel, 250 mg Acetyl-salicylic acid (ASA), 100 U/kg unfractionated heparin (UFH) associated with high dose of statin and i.v. nitrate the patient’s chest pain disappeared. Primary PCI was elected, revealing occlusion of the left descendent artery in the second segment, which was treated with a drug eluting stent angioplasty. The post PCI evolution was favorable with no recurrent chest pain and no signs of heart failure, on classic treatment. Keywords: Left anterior descending artery (LAD) occlusion, De Winter T waves, acute coronary syndrome, primary percutaneous coronary intervention (PCI)
INTRODUCTION
The De Winter syndrome is characterized by ST depression and peaked T waves in precordial leads. Some authors consider this pattern to be an equivalent of anterior STEMI2.
CASE REPORT
We report the case of a 41 years old male admitted three hours after the onset of typical angina associated with profuse sweating. The patient was a heavy smoker (40 PA) and he had no other known cardiovascular risk factors, but he had a positive family history for cardiovascular disease. Upon admission the patient was in severe pain, but otherwise stable. The fi rst ECG revealed sinus rhythm, 80 bpm and 2 mm upsloping ST segment depression with tall and peaked symmetric T waves in the precordial leads V3-V4 resembling De Winter’s pattern (Figure 1). The first and the second troponin I values taken one hour and four hours from the onset of the pain were negative (0.003 ng/ml and 0.087 ng/ml, respectively). The patient was initially managed conservatively on pharmacological treatment with disappearance of the pain after a 3 μg/min dose of i.v. nitroglicerin was initiated. An echocardiogam was performed and revealed akinetic interventricular septum, apex and apical inferior wall with a global ejection fraction of 40% and a mild mitral regurgitation. Subsequent ECG tracings revealed R waves amputation and notching in the downslope of the S wave in leads V1 through V4 (Figure 2). A third determination of the troponin I taken 11 hours from the onset of pain was above the cut-off for myocardial necrosis (4.14 ng/ml) and we decided then to alert the cath lab. Coronary angiography revealed monovasal disease with 100% stenosis of the left descendent artery in the second segment (Figure 3). After thrombus aspiration a DES
stent was implanted with primary procedural success (3.5/33 mm DES with postdilation with noncompliant balloon) (Figure 4 and 5). The post PCI ECG revealed the normalising ST segment and negative T waves in V2-V4 leads, together with potential loss in V1-V4 leads, proving the anterior necrosis (Figure 6). The postangioplasty course was uneventful and the patient was discharged on day 4.
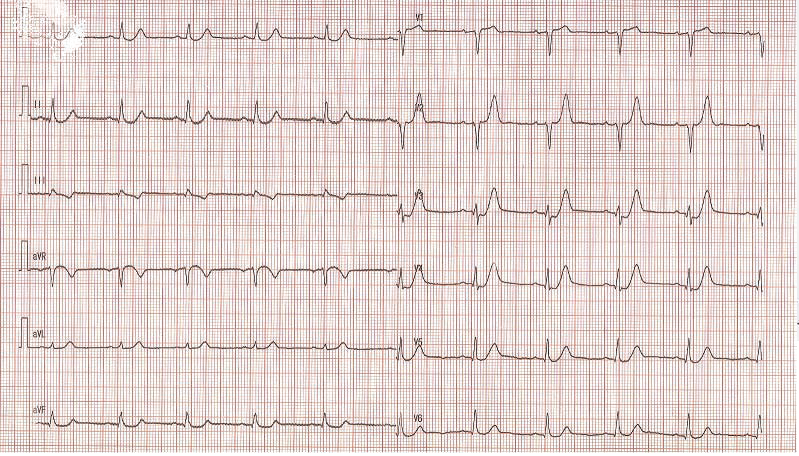
Figure 1. ECG: sinus rhythm, 80 bpm and 2 mm upsloping ST segment depression with tall and peaked symmetric T waves in the precordial leads V3-V4 resembling De Winter’s pattern.
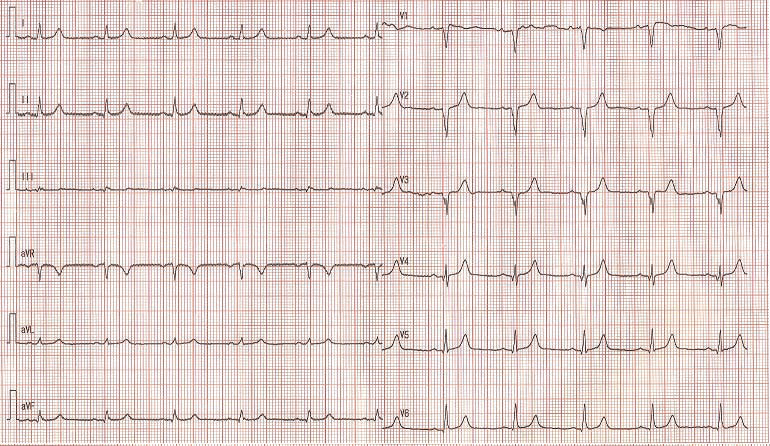
Figure 2. ECG tracings revealed R waves amputation and notching in the downslope of the S wave in leads V1 through V4.
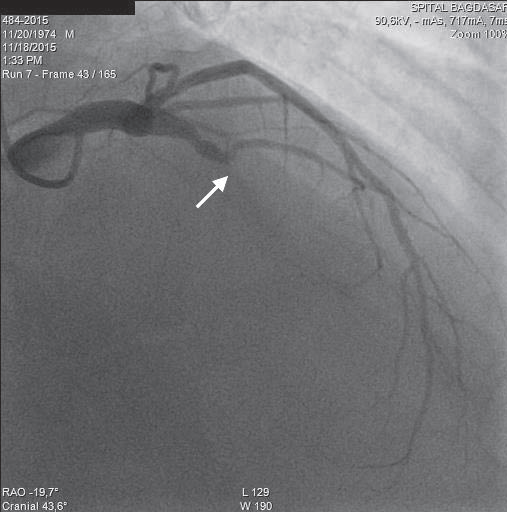
Figure 3. Coronary angiography: left descendent artery in the second segment (LAD) occlusion (see arrow) – OAD Cranial incidence.
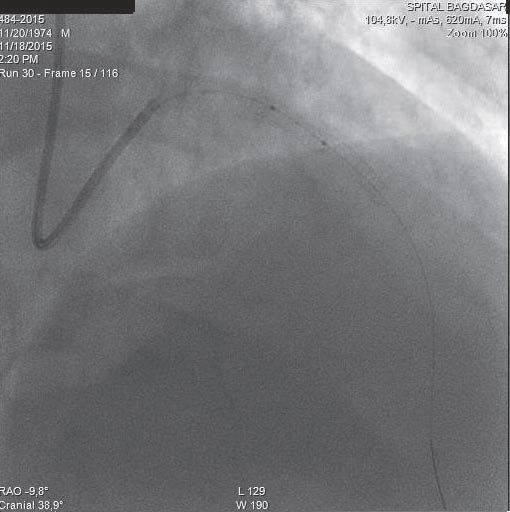
Figure 4. Coronary angiography. Instent postdilation.
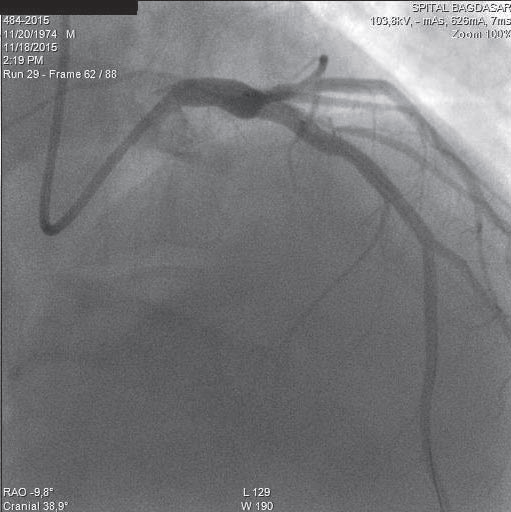
Figure 5. Coronary angiography: Coronary angiography
DISCUSSIONS
The De Winter ECG pattern was fi rst taken into consideration in 2008 in a case series by De Winter and Wellens which observed this in 30/1532 patients presented with acute LAD occlusions (2%)1. In another case series Verouden et al. found this pattern in 35/1890 patients requiring PCI for LAD occlusions. In this series the patients were younger, had a higher incidence of hypercholesterolemia and were more often male than the rest of the patients presented with ST elevation anterior myocardial infarction3. This finding may be useful for an invasive strategy in these patients which may lead to a better short and long term prognosis. As urgent reperfusion therapy is indicated to patients presenting with ST elevated myocardial infarction, patients
with ST depression on admission benefit from this urgent therapy only in some cases. Patients with hemodynamic instability or electrical instability, with acute mitral regurgitation, with acute severe LV dysfunction or with persisting symptoms on best medical treatment are some of these patients. Nevertheless, patients with multilead ST depression and ST elevation in aVR may benefi t also from urgent reperfusion therapy as this has been reported in patients with myocardial infarction and occlusion of the left main artery, occlusion of the proximal left anterior descending artery
or in the presence of severe multivessel coronary artery disease4. All these prove the need for an updated defi nition of ECG signs of coronary artery occlusion – especially LAD occlusion –, as many patients may benefit from acute invasive treatment instead of conservative strategy.
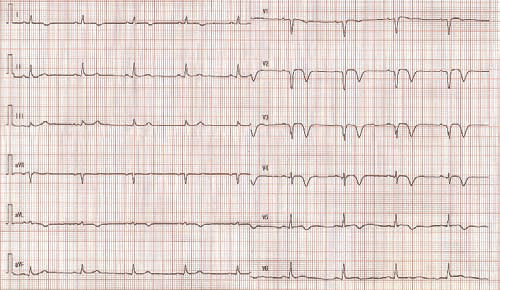
Figure 6. PCI ECG – the normalising ST segment and negative T waves in V2-V4 leads, together with potential loss in V1-V4 leads, proving the anterior necrosis.
CONCLUSIONS
De Winter syndrome is a rare occurrence, but signals an extremely severe coronary pathology with a high mortality. Rapid recognition of this syndrome may help for early treatment of these patients, which means often percutaneous coronary revascularization. Conflict of interests: none declared.
References
1. Goebel M, Bledsoe J, Orford JL, Mattu A, Brady WJ. A new ST-segment elevation myocardial infarction equivalent pattern? Prominent T wave and J-point depression in the precordial leads associated with ST-segment elevation in lead aVr. Am J Emerg Med. 2014 Mar;32(3):287.
2. De Winter R, Verouden N, Wellens H, Wilde A. A new ECG sign of proximal LAD occlusion. N Engl J Med 2008;359:2071–3.
3. Verouden NJ, Koch KT, Peters RJ, et al. Persistent precordial “hyperacute” T-waves signify proximal left anterior descending artery occlusion. Heart 2009;95:1701–6.
4. Fesmire F, Hennings J. A new electrocardiographic criteria for emergent reperfusion therapy. Am J Emerg Med 2012;30:994–1000.
 This work is licensed under a
This work is licensed under a