Miruna Ocos2, Lucian Petrescu1,2, Cristina Vacarescu1, Cristian Mornos1,2, Emilia-Violeta Goanta3, Simina Crisan1,2, Oana Patru2, Nicolae Catalin2, Dragos Cozma1,2
1 Institute of Cardiovascular Diseases, Timisoara, Romania
2 „Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania
3 Department of Cardiology, Emergency County Hospital Craiova, Romania
Abstract: Introduction – Situs inversus totalis is a rare congenital malformation, diagnosed at about 1 from 10.000 of patients. It’s diagnosis is usually made incidentally. Case report – Female patient, 46 years old, diagnosed with dextrocardia at the age of 16 based on chest X ray, is referred to our clinic for assessement of one sincopal episode. The ECG trace at admission revealed sinus bradycardia, a heart rate of 35 beats per minute, negative T waves in precordial leads V1,V2. Tran-sthoracic echocardiography revealed concordant atrioventricular and ventriculo-arterial connections, normal size for both ventricles, normal biventricular function and mild tricuspid regurgitation. A dual pacemaker was performed, with favorable evolution. Disscusions – Limited data about patients with situs inversus totalis and rhythm/conduction disorders, makes more difficult their management, being fundamental to make a correct diagnosis. The implantation technique of a patient with dextrocardia can be a very challenging one.
Keywords: situs inversus totalis, rhytm/conduction disorders, dextrocardia.
INTRODUCTION
Situs inversus, a rare congenital malformation, descri-bed for the first time by Matthew Baille. It is an auto-somal recessive genetic condition, but sometimes it can be X-linked. The term situs inversus, short form of the Latin “situs inversus viscerum” describes the in-verted position of abdominal and chest organs. When associated with dextrocardia is referred as situs in-versus totalis1. There are also cases of situs inversus with levocardia, these are rare and 95% of them are associated with congenital heart diseases, most com-monly transposition of great vessels2. About 25% of individuals with situs inversus can have primary ciliary dyskinesia, the so called Kartagener syndrome, cha-racterized by bronchiectasis and chronic sinusitis3. Generally individuals are asymptomatic, unaware of their anatomical variation, being diagnosed by mistake.
CASE REPORT
A 46 year old, female patient, diagnosed with dextro-cardia at the age of 16 based on X-ray fluoroscopy, was reffered to our clinic for assessment of one synco-pal episode. In addition she was diagnosed with situs inversus totalis 3 years ago. Her physical examination was normal, with resting blood pressure in left arm of 120/60 mmHg and a heart rate of 35 beats per minute at rest. On cardiovascular examination, the apex was present in the 6th intercostal space on the right side, lateral to mid clavicular line, rhythmic heart sounds, without murmurs.
The ECG trace at admission revealed sinus bra-dycardia, a heart rate of 35 beats per minute, a QRS axis of 0 grd, narrow QRS complexes and negative T waves in precordial leads V1-V2 (Figure 1). The bio-logic investigations revealed high levels of triglyceride. Transtoracic ecocardiography showed mirror image dextrocardia, concordant atrioventricular and ventri-culo-arterial connections, normal size for both ven-tricles, EF 55%, normal function of the right ventricle (TAPSE of 23 mm) and mild tricuspid regurgitation (Fi-gure 2). During her hospitalization we made two Hol-ter monitoring that revealed severe bradycardia with junctional escape rythm; a medium heart of 30 beats/ minute, numerous sinus pauses grater than 3000 ms, the maximum of 5000 ms, numerous isolated prema-ture ventricular contractions and systematized, with maximum length no more than 5 complexes. It is im-portant to emphasize that the patient was paucysimp-tomatic during her monitorization. At the stress test, the patient achieved 125 W, maximum heart rate was 76 beats/minute (only 44% of her target), that showed a chronotropic incompetence; without induction of nonsustained or sustained tachyarrithmias during all stages.
Considering that the patient had a family history of sudden death (father deceased at age 49), the suspicion of arrhytmogenic right ventricular dysplasia (ARVD) was rised, so we had to establish whether the patient has indication for an implantable cardio-verter defibrillator or a pacemaker. We so performed an MRI, the sistolic and diastolic function of both ven-tricles were normal, also the absence of fibro-fatty inflammation afecting the right ventricle helped us to rule out the diagnosis of ARVD. The MRI showed the total transposition of abdominal and thoracic viscera (the so called mirror image of the internal organs nor-mal positioning) (Figure 3). We managed also to exclu-de different structure cardiac anomalies which can be associated with dextrocardia such as interventricular defects, transposition of the great vessels4. Therefore according to „2015 ESC Guidlines on cardiac pacing and resyncronization therapy” our patient has class I indication, level of evidenc C for pacemaker (PM) implant. The next day, under antibiotic protection, a dual chamber PM was implanted, using the left sub-clavicular vein access. Through the left superior vena cava, two pasive leads were implanted, one in the right ventricular apex and one in the right atrial appendage; the senses and threshold parameters were appropri-ate (Figure 4). Regarding the implantation technique, there is no clear recommendation in this case, being more a choice of the interventional cardiologist. The-re were no complications during and after the inter-vention. The pacemaker was programmed DDDR 60 beats per minute, we optimized the atrioventricular interval (a long AV delay) in order to allow the intrin-sec conduction and to minimize the right ventricular pacing. A post procedural 12 lead ECG trace showed atrial pace and ventricular sensed complexes (Figure 5). As treatment we recommended antihypertensive therapy with a combination of converting enzyme in-hibitor and diuretic tiazidic like (Perindoprilum/Inda-pamidum 5/1,25 mg a day), fenofibrate 145 mg a day.

Figure 1. The electrocardiogram performed at admission-sinus brady-cardia, narrow QRS complexes and negative T waves in precordial leads V1-V2.
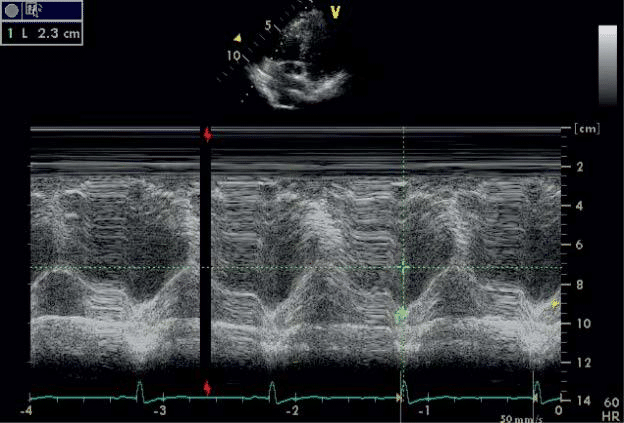
Figure 2. Tricuspid annulus systolic excursion of 23 mm.
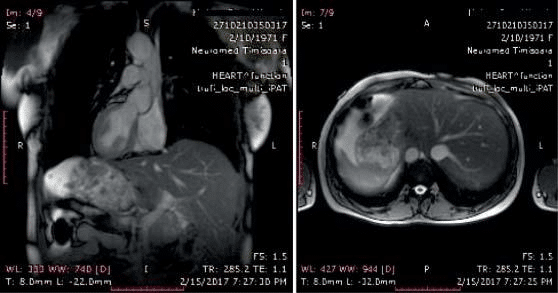
Figure 3. Mirror image of the internal organs normal positioning.
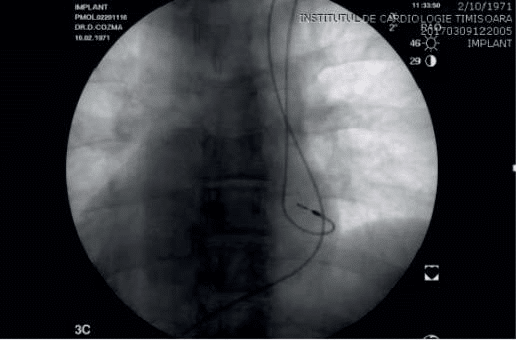
Figure 4. Through the left superior vena cava, two leads were implanted, one in the right ventricular apex and one in the right atrial appendage.
CONCLUSIONS
Limited data about patients with situs inversus totalis and rhythm/conduction disorders, makes more diffi-cult their management, being fundamental to make a correct diagnosis because of their individual anatomy.
The implantation technique of a patient with dextro-cardia can be a very challenging one, that is why before the procedure it is important to gather informations about the anatomy and the pressence or absence of congenital abnormalities, very common at this pati-ents5,6. As far as we know, few cases with situs inver-sus totalis who were implanted using the left vascular access were reported in literature, our patient being one of them.
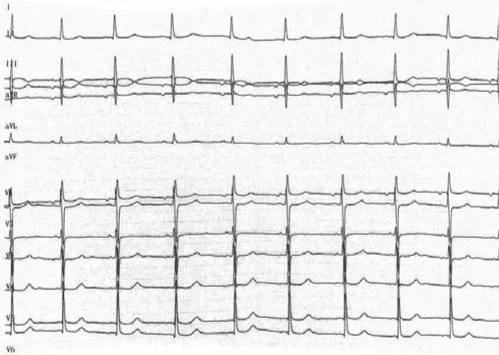
Figure 5. Post procedural 12 lead ECG trace.
Conflict of interest: none declared.
Authors’ contributions: Concept/design: OM, CV, DC, LP; Data collection: OM, CV, CN, OP Data analysis/interpretation: DC, CM, SC; Drafting article: OM, CV, CN, EVG, SC; Critical revision of article: LP, CM, DC.
Abbreviations
ARVD arrhytmogenic right ventricular dysplasia
MRI magnetic resonance imaging
PM pacemaker
TAPSE tricuspid annulus planse systolic excursion
EF ejection fraction
References
1. Evans WN, Acherman RJ, Collazos JC, et al. Dextrocardia: practi-cal clinical points and comments on terminology. Pediatr Cardiol 2010;31:1–6..
2. Atehef Ghornazadeh, Nahid Zirak, Afsoon Fazlinezhad- Situs Inver-sus with Levocardia and Congenitally Corrected Transposition of Great Vessels in a 35 year old Male: A Case report, Electron Physi-cian. 2017 January; 9(1): 3570–3574.
3. Babaji Ghewade, Smaran Claudius, Swapnil Chaudari, Arvin- A Case of Kartagener with Pulmonary Hypertension, Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online.
4. Yener N, Surucu HS, Dogan R, et al. A case with dextrocardia, ven-tricular septal defect, persistent left superior vena cava and drainage of the great cardiac vein into the left internal thoracic vein. Surg Ra-diol Anat 2001;23:205–6.
5. Dextrocardia- H.G. Mond, P.P. Karpawich (Eds.), Pacing options in the adult patient with congenital heart disease, Blackwel Publish-ing, Massachusetts (2007) 10.1002/9780470750940.ch18
6. N.A. Estes 3rd, D.N. Salem, J.M. Isner, et al.Permanent pacemak-er therapy in corrected transposition of the great arteries: analysis of site of lead placement in 40 patients. Am J Cardiol, 52 (1983), pp. 1091-1097.
 This work is licensed under a
This work is licensed under a