Anca Mateescu2, Monica Roşca1,2, Carmen Ginghină1,2, B. A. Popescu1,2
1 University of Medicine and Pharmacy “Carol Davila” Bucharest, Laboratory Euroecolab
2 “Prof Dr C.C. Iliescu” Institute of Emergency for Cardiovascular Diseases, Bucharest
Contact address:
Bogdan A. Popescu, MD, PhD, University of Medicine and Pharmacy “Carol Davila”, Euroecolab, “Prof Dr C.C. Iliescu” Institute of Emergency for Cardiovascular Diseases, Sos Fundeni No. 258, 022322 Bucharest
E-mail: bogdan.a.popescu@gmail.com
A 66 year old woman with atrial septal defect (ASD) diagnosed in childhood and without proper follow-up was admitted for fatigue at small effort and palpitations. The physical examination revealed an irregular pulse, 115 beats/min, blood pressure of 110/70 mmHg, a second degree systolic murmur at the left sternal border and peripheral edema. On the ECG atrial fibrillation (112 bpm), right axis deviation and right bundle branch block are identified. The transthoracic echocardiogram (TTE) shows an ostium secundum ASD (maximum diameter of 26 mm) (Figure 1) with significant left-to-right atrial shunt, right atrial and right ventricle enlargement, paradoxical interventricular septal motion, moderate-severe secondary tricuspid regurgitation, pulmonary hypertension (systolic pulmonary artery pressure estimated of 65 mmHg) and significant dilation of the pulmonary artery trunk. TTE also reveals mild-moderate mitral regurgitation, severely dilated left atrium, normal dimensions of the left ventricle (LV) with a preserved global LV function, and a small pericardial effusion. A 3-dimensional (3D) TTE was performed in order to delineate the morphology and shape of the ASD. The 3D “en face” view of the ASD was obtained (Figure 2). The echo size of the ASD measured from the 3D image was 21 x 29 mm, with sufficient rims surrounding the defect, making it anatomically feasible for device closure. The transesophageal echocardiogram (TEE) confirmed the ostium secundum ASD with left-to-right shunt. ASD rim measurements at TEE agreed fairly well with 3D TTE (Figure 3).
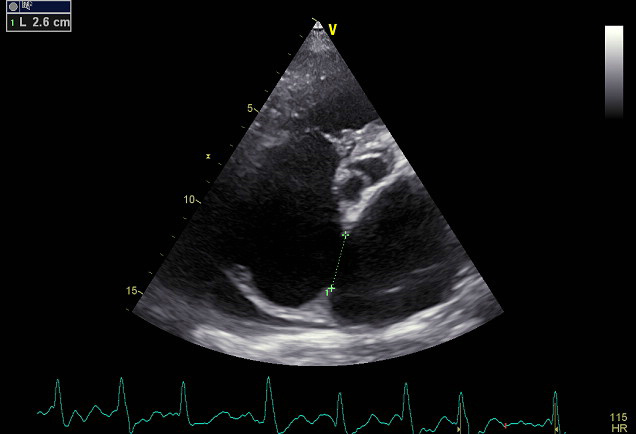
Figure 1. TTE examination, modified 4 chamber view, reveals an ostium secundum ASD with a maximum diameter of 26 mm.
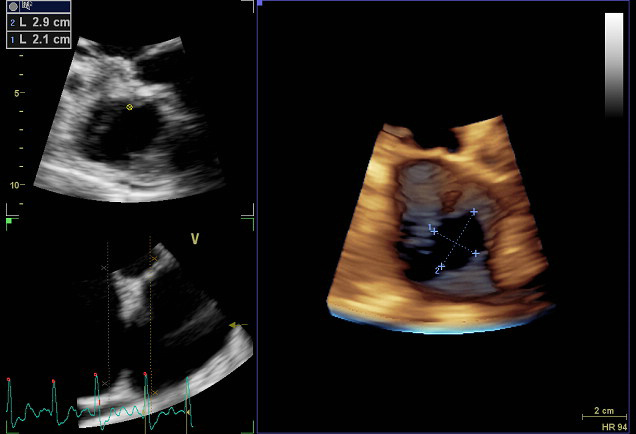
Figure 2. 3-dimensional TTE. “En face” volume rendering view of the ASD (right panel) visualised from the left atrium, with 29/21 mm diameters.
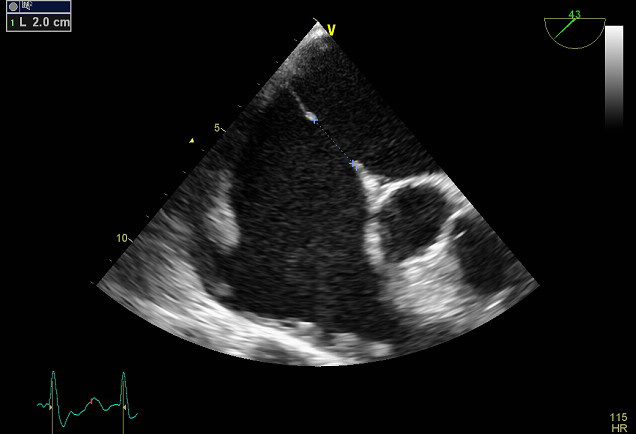
Figure 3. TEE exam confirms the ostium secundum ASD with a maximum diameter of 20 mm in this view.
Prior to referring a patient with ASD for percutaneous device closure the proper assessment of defect anatomy is mandatory. Three-dimensional TTE is a non-invasive method allowing the accurate determination of ASD location, size and shape, and characterization of its borders.
Conflict of interest: none declared.
References:
1. García-Fuertes D, Mesa-Rubio D, Ruiz-Ortiz M, et al. Monitoring complex secundum atrial septal defects percutaneous closure with real time three-dimensional echocardiography. Echocardiography 2012;
29:729-34.
2. Acar P, Aggoun Y, Le Bret E, et al. 3D-transthoracic echocardiography: a selection method prior to percutaneous closure of atrial septal defects. Arch Mal Coeur Vaiss. 2002; 95:405-10.
3. van den Bosch AE, Ten Harkel DJ, McGhie JS, et al. Characterization of atrial septal defect assessed by real-time 3-dimensional echocardiography. J Am Soc Echocardiogr 2006; 19:815-21.
 This work is licensed under a
This work is licensed under a