Alexandrina Nastasa1, Mohamed Dardari1, Radu Vatasescu1
1 Clinical Emergency Hospital, Bucharest, Romania
Abstract: Curative radiofrequency catheter modification of the slow pathway is the recommended therapy for atrioventricular nodal reentry tachycardia (AVNRT) which is usually performed via femoral vein through inferior vena cava (IVC) approach. Diagnostic and ablation procedures are diffi cult when this approach is not possible due to congenital or acquired obstruction of the IVC. Here, we report a case with IVC anomaly (left IVC with interruption after receiving the renal veins and hemi-azygous continuation) in whom AVNRT ablation was achieved without complications via the azygous system using a remote-controlled magnetic navigation system.
Keywords: magnetic navigation system, ablation procedure, congenital malformation
INTRODUCTION
Curative radiofrequency catheter modification of the slow pathway is the recommended therapy for atrioventricular nodal reentry tachycardia (AVNRT) which is usually done through inferior vena cava (IVC) approach. Problems may arise when this approach is not possible due to congenital or acquired obstruction of the IVC. Although a superior access6 (jugular1,3 or subclavian2)
has been proposed as an alternative, these ablation approaches are associated with increased fluoroscopy radiation exposure for the operator, less comfort for both the patient and the operator, poor manoeuvrability and a lower catheter stability. Advancing the catheter manually through the azygous system has been previously reported in one case with azygos continuation using a hypoplastic but uninterrupted IVC5 and one case with IVC interruption, where venous return drained into the azygos system and a transseptal sheath was placed through the venous anomaly for the advancement of the ablation catheter4. To the best our knowledge remote magnetic navigation was not used for such approach before. We describe a case with IVC anomaly (left IVC with interruption after receiving the renal veins and hemiazygous continuation) in whom AVNRT ablation was achieved without complications through the azygous system using a remote-controlled magnetic navigation system.
CASE SUMMARY
A 48-year-old obese female with a history of reccurent symptomatic supraventricular tachycardia in the absence of structural heart disease was reffered for ablation. History revealed that in 2008 she had a previous ablation attempt in another centre that failed because it was impossible to advance the ablation catheter inside the heart via femoral approach (only one thin diagnostic catheter (5F) was advanced). Although it was assumed that the patient had IVC occlusion no diagnostic workup was performed. Physical examination was unremarkable. ECG during tachycardia showed narrow QRS with no retrograde p- waves, at the rate of 180 beats/min with ECG in sinus rhythm being normal (no delta waves). The echocardiography was also suggesting IVC occlusion. There was also a turbulent flow located at the SVC, just superior to SVC-RA junction. Subsequently a CT angiogram was performed, that documented that IVC was formed on the left side of the aorta and was interrupted after receiving the renal veins with venous drainage into the hemiazygous-azygous system, then superior vena cava and right atrium. There was no segment of the inferior vena cava between the renal veins and the suprahepatic veins which formed a common trunk that drained directly into the right arium. The CT also showed multiple bilateral small pulmonary emboli (asymptomatic discovery). Oral anticoagulation with NOAC (Apixaban 5 mg x 2/day) was then initiated and continued for one month before the procedure. The ablation procedure was performed with uninterrupted anticoagulation. Initially a 5F decapolar diagnostic catheter was positioned in the coronary sinus (CS) through the left subclavian vein. The clinical tachycardia was easily induced with programmed electrical stimulation, initially with a RBBB aberancy then with a narrow QRS and an activation sequence typical to atrioventricular nodal re-entry tachycardia (Figure 3). Arrhythmia was then terminated with overdrive pacing. The right femoral vein was cannulated and a RMT ablation catheter (Celsius RMT ThermoCool, 8F, spacing 2-5-2) was introduced (Stereotaxis Inc, Niobe II). As the catheter was introduced using remote magnetic navigation, it passed on left side of the spine (via hemiazygous vein) as it is shown in Figure 4. Afterwards the catheter was advanced to the right side of the spine into the azygos vein, then passing into the superior vena cava (SVC) and subsequently looped into the right atrium as ilustrated below. A slow pathway potential was documented in sinus rhythm and then radiofrequency (56 degrees, 50 watts) applications were delivered, resulting in an accelerated junctional rhythm. Thereafter, programmed atrial stimulation demonstrated the elimination of the slow pathway conduction, and it did not induce any other SVTs. The entire procedure (patient preparation included) took 65 minutes, of which 7 minutes of fluoroscopy and 3 minutes cumulative RF application time. No complications occurred.
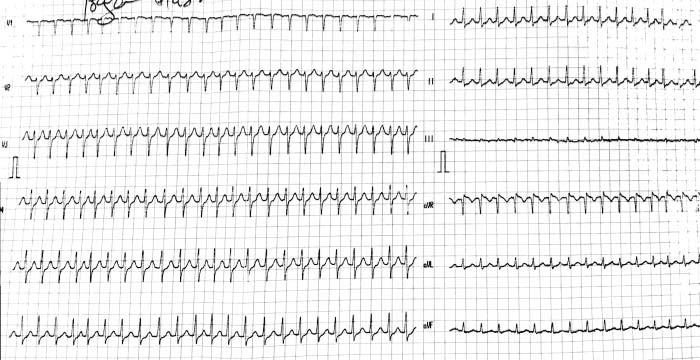
Figure 1. ECG with narrow QRS tachycardia.
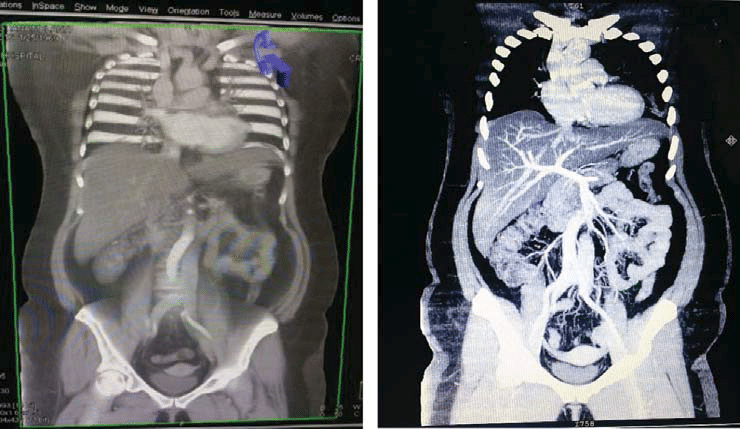
Figure 2. CT angiogram showing left IVC interrupted after renal level; also visible on the right panel suprahepatic trunck draining in the right atrium.
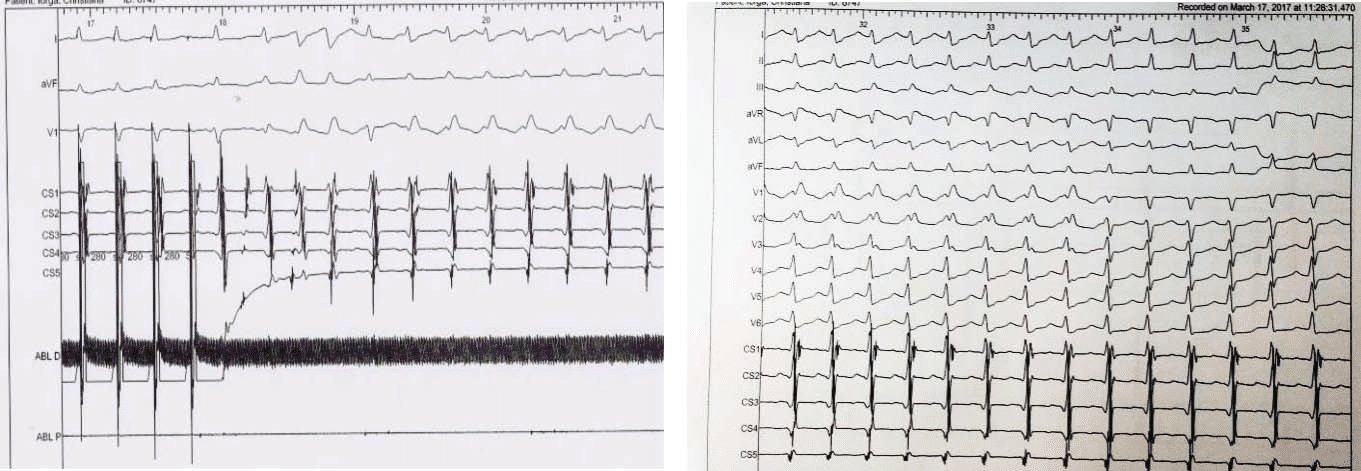
Figure 3. Programmed electrical stimulation inducing clinical tachycardia, left panel – CS activation suggesting AVNRT, right panel – surface ECG showing initial RBBB aberrancy, then narrow QRS.
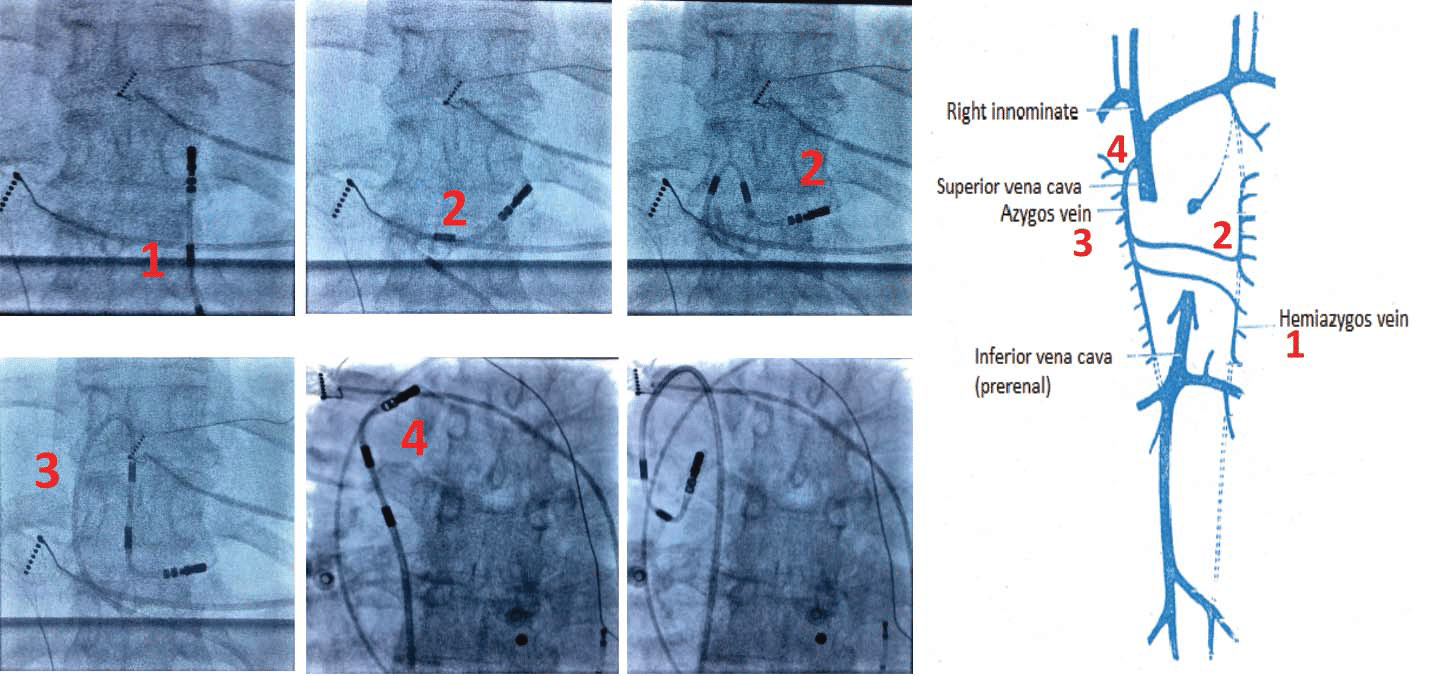
Figure 4. Passage of the ablation catheter: on the left side: 1, 2 in the hemiazygous vein, 3 in the azygous vein, 4 at the junction with the superior vena cava.
DISSCUSSION
Incidence of IVC interruption in the general population is 0.1-0.6%7. The manipulation of the catheters through the azygos continuation of the IVC was described previously in patients with congenital IVC anomalies4,5 but it was difficult and time-consuming, because of its long course and angulation, often not allowing His or slow pathway potential localisation. In our case a stable His bundle electrogram was obtained without great difficulty and the RMT catheter had good stability in the slow pathway region (Figure 6). It is important to mention that having a catheter with a soft consistency like Celsius RMT offers a great manoeuvrability in such complicated approach, with practically no risk of perforation. The superior approach (jugular, subclavian) that was previously used in similar cases could have posed serious risks in an obese patient (pneumothorax, arterial puncture etc.) that were minimised in our case by using only one subclavian puncture for a thin diagnostic catheter (5F). The significant discomfort and risks (increased X-ray exposure for the operator, increased risk of desterilization), of manipulating the ablation catheter in the jugular or subclavian vein were also avoided. The jugular and subclavian veins have been proposed as an alternative approach for the ablation catheter in such cases, however, the potential drawbacks of a superior access could be the poor orientation and poor manoeuvrability of the ablation catheter and lower catheter stability, which are essential to avoid complications such as complete AV block. The actual risk of manual manipulation of the ablation catheter thorugh jugular/subclavian approach is even higher if we consider how exceptionally rare electrophisiologista use this approach. An overestimated disadvantage could be represented by the non-significant increased procedural costs, which is actually not an important issue if someone considers the low incidence of this anomalies. However a carefull analysis of risk / benefit ratio should be performed in each case.
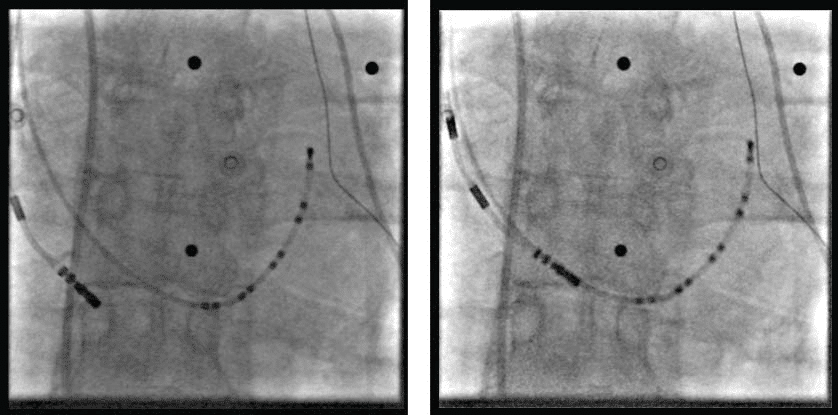
Figure 5. Diagnostic catheter (decapolar) in the coronary sinus (via left subclavian vein) and the ablation catheter in the right atrium via azygous – SVC.
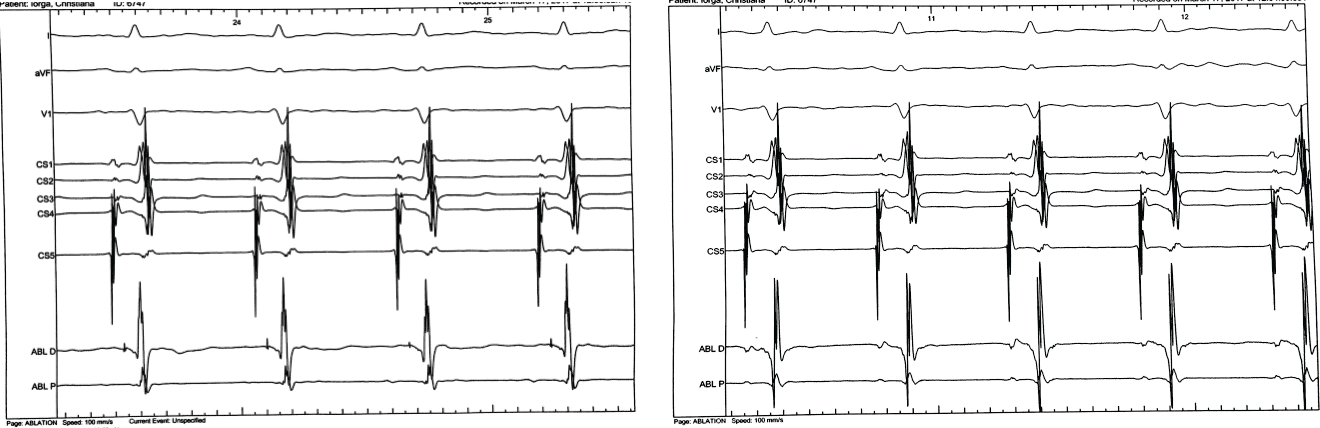
Figure 6. Intracardiac electrograms: His electrogram (left panel), slow pathway potential (right panel).
CONCLUSION
An inferior venous approach via hemiazygous-azygos system can be easily obtained in patients with IVC obstruction due to increased catheter flexibility and steering accuracy of the remote magnetic navigation system.
Conflict of interest: none declared.
References:
1. Kelesidis I., Palma E., “Catheter Ablation of Atrial Flutter in a Patient with Azygos Continuation of the Inferior Vena Cava after Failed Surgical Cryolesions” The Journal of Innovations in Cardiac Rhythm Management, 3 (2012), 1011–1014
2. Machado C., Liddon V., Roy D. ”Radiofrequency catheter ablation of fast pathway via unconventional right subclavian venous access for atrioventricular reentrant tachycardia. J. Interv Cardiol 2003; 16: 377- 380.
3. Karthigesan M., Jayaprakash S. “Radiofrequency Catheter Ablation Of Atrioventricular Nodal Reentry Tachycardia In A Patient With Inferior Vena Cava Anomaly” Indian Pacing and Electrophysiology Journal. 2009;9(4):214-218.
4. Randhawa SM., Taylor HC., Mosteller RD. “Anatomic Twist to a Straightforward Ablation” Indian Pacing Electrophysiol J. 2013 Mar-Apr; 13(2): 94–98.
5. Arbelo E., Caballero E., Medina A. “Successful slow pathway ablation for atrioventricular nodal re-entrant tachycardia via a hypoplastic inferior vena cava in a patient with an azygos continuation” Europace. 2008 Apr;10(4):467-8.
6. Yamada T., McElderry TH., Kay N. “Radiofrequency catheter ablation of the slow pathway for atrioventricular nodal reentry in a patient with an obstructed inferior vena cava” J Interv Card Electrophysiol (2008) 22:195–198
7. Trigaux JP, Vandroogenbroek S, De Wispelaere JF, Lacrosse M, Jamart J. Congenital anomalies of the inferior vena cava and left renal vein: evaluation with spiral CT. J Vasc Interv Radiol 1998; 9:339–45.
 This work is licensed under a
This work is licensed under a