Ionut Badescu1, Freddy Frost1
1 Liverpool Heart and Chest Hospital, Liverpool, United Kingdom
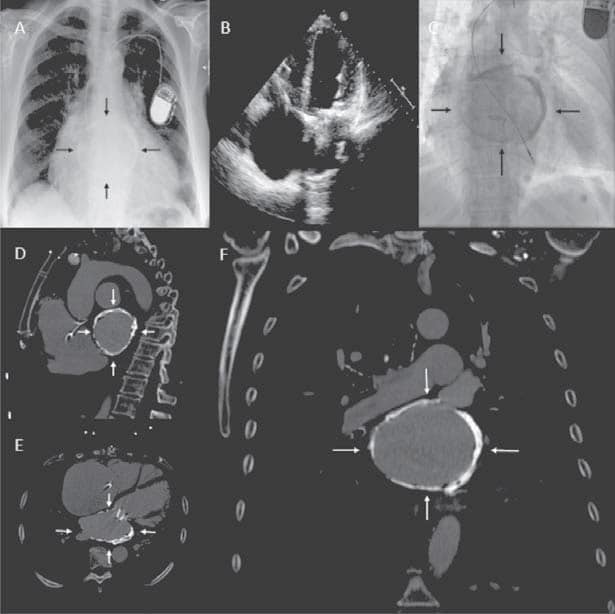
We report the case of a 71 year old lady who presented with increasing breathlessness, palpitations and leg swelling. Her past medical history included rheumatic fever with metallic mitral and aortic valve replacements, atrial fibrillation and a permanent pacemaker for symptomatic bradycardia. CXR (Panel A) demonstrated clear lung fields but a dense calcification in the mediastinum. Transthoracic and transoesophageal echocardiography (Panel B) were both sub-optimal and assessment of the metallic valves, ventricular function or calcification was not possible. Fluoroscopy (Panel C) was pursued to assess the mechanical function of the valves, which were shown to be mechanically sound, but the calcification could not be characterised further. CT Chest (Panel D, E & F) was performed and revealed a heavily calcified left atrium with septal sparing in keeping with a diagnosis of porcelain atrium. Porcelain atrium is a rare finding associated with rheumatic heart disease. The clinical significance is often minimal with few directly attributable sequelae. However, if further surgical intervention is required to the mitral valve, the atrial calcification poses a risk of major complications as a source of emboli and impaired haemostasis. Our patient’s symptoms were attributable to a dehiscence of her aortic valve replacement and hence she was referred for re-do aortic valve surgery.
Conflict of interest: none declared.
 This work is licensed under a
This work is licensed under a