Teodora Nita1, Paula Gocan1, Ioana Dregoesc1, Svetlana Encica2, Lucian Stan3, Ruxandra Beyer1
1 Department of Cardiology, Heart Institute “Niculae Stancioiu”, Cluj-Napoca, Romania
2 Department of Anatomic Pathology, Heart Institute “Niculae Stancioiu”, Cluj-Napoca, Romania
3 Department of Cardiovascular Surgery, Heart Institute “Niculae Stancioiu”, Cluj-Napoca, Romania
Abstract: Cardiac myxomas are rare benign tumors generally located at the border of fosa ovalis in the left atrium. Cli-nical presentation may vary and overlap with other cardiovascular disease, so echocardiography is necessary for diagnosis. We describe the clinical case of a 58-year-old woman with chronic exertional dyspnea diagnosed with left atrial myxoma based on transthoracic echocardiography. Severe mitral valve obstruction and regurgitation by the large tumoral mass had important hemodynamic consequences leading to severe pulmonary hypertension. Complete surgical resection was perfor-med and histopathological examination confirmed the diagnosis. Keywords: left atrial myxoma, dyspnea, echocardiography, mitral valve
INTRODUCTION
The heart is the source of both primary and secondary tumors. Any form of cancer can determine metastases in the heart, 20 to 40 fold more frequent than pri-mary tumors1. About 75 percent of primary tumors are benign, the most frequent are myxomas with typi-cal localization in the left atrium2. Other localization of myxomas have been described: right atrium3, ven-tricles4, inferior and superior cava veins5, Eustachian valve6, femoral vein7.
CLINICAL MANIFESTATIONS
Clinical manifestation depend on the size and position of the tumor and can be classified as follows: symp-toms due to mechanical obstruction and/or valve in-volvement, as well as due to the direct invasion of the myocardium (cough, dyspnea, thoracic pain, dizziness, palpitations, syncope, circulatory collapse), constitu-tional symptoms (weight loss, pyrexia of unknown origin, malaise) and embolic symptoms mainly in the central nervous system8.
CASE REPORT
A 58 year-old woman with medical history of hypothy-roidism presented in the outpatient department for chronic exertional dyspnea. Clinical examination re-vealed blood pressure 100/80 mmHg, pulse rate 101 bpm and a holosystolic murmur at the apex of the hearth. Auscultation of the lung was normal bilaterally and no jugular vein distention was presented. Pulses were intact bilaterally with no peripheral oedema and there were no neurological defi cits. Electrocardiogram revealed normal sinus rhythm with minor right bundle branch block (Figure 1). Transthoracic echocardio-gram showed a large echogenic mass of 53/31mm in the enlarged left atrium (54/81 mm) attached to in-teratrial septum (Figure 2). The tumor area was 16.8 cm2, homogeneous and mobile with protrusion into the left ventricle during diastole, causing severe mitral regurgitation and stenosis (Figure 3). The left ventricle ejection fraction was normal. The right ventricle was slightly enlarged, the systolic pulmonary pressure was estimated at 70 mmHg.
The patient was referred to another hospital for further investigations and surgical treatment. On ad-mision, laboratory fi ndings were near normal: WBC 11510/μl, Hb – 13.3 g/dl, Hct – 39.6%, Platelets – 161000/μl, Na – 145 mmol/l, K – 5 mmol/l, Urea – 31.1 mg/dl, Creatinine – 0.75 mg/dl, ALT – 15UI/l, AST – 23UI/l, TSH – 1.45 μUi/ml, FT4 – 0.98 ng/dl, prothrombin time – 12.4 sec. The coronary angiogra-phy was normal. The patient was promptly transferred to Cardiovascular Surgery Department and underwent resection of the left atrium tumor. Intraoperative the heart motion was adequate with enlarged left atrium. The tumor was friable, implanted on the interatrial septum, had 60/40 mm diameters, suggesting an atrial myxoma (Figure 4). The atrial wall was reconstruc-ted with a bovine pericardial patch. The diagnosis of myxoma was confirmed by the histological exams (Fi-gure 5 and 6). Early postoperative recovery was good, with removal of the drainages the following day. Five days later the patient presented rapid onset of pal-pitations, dyspnea with orthopnea. Electrocardiogram showed atrial fibrillation. Conversion to normal sinus rhythm was obtained using intravenous amiodarone. Chest X-Ray reveled moderate right pleural effusion and pleural drainage was made for 24 hours. After 13 days the patient was discharged asymptomatic on beta-blocker, propafenone, diuretics, H2-blocants, le-vothyroxine and vitamin K antagonists.
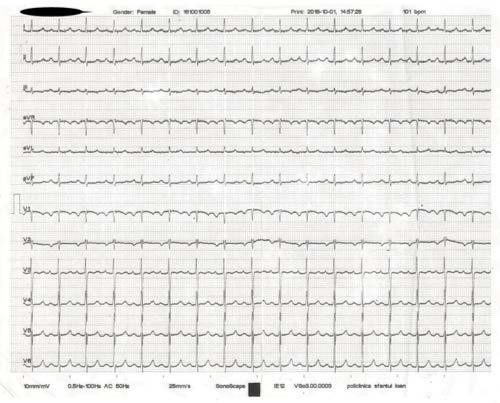
Figure 1. Sinus tachycardia.

Figure 2. Transthoracic echocardiography shows a large mass filling left atrium (parasternal long axis).
DISCUSSION
Clinical presentation, diagnosis and treatment of car-diac tumors can be very challenging. In our patient the symptoms were caused by se-vere pulmonary hypertension due to the prolapse of the tumor in to the left ventricle during diastole with severe mitral obstruction and to the mitral regurgi-tation. Transthoracic echocardiography (TTE) is the initial test in a patient suspected with cardiac tumor. Left atrial myxomas are usually hyperechoic, well delimited tumors located at the border of the fossa ovalis. Echocardiography identifies the tumor, the im-plantation base and may be helpful to determine the mobility and the relation with the mitral valve. Tran-soesophageal echocardiography has better sensitivity and specificity than transtoracic echocardiography for cardiac myxoma. In our patient, the TTE was suffi ci-ent in confirming the diagnosis. Differential diagnosis must be primarily made with thombus. Contrast com-puted tomography (CT), cardiac magnetic resonance imaging (MRI) and positron emission tomography-CT may be useful in this situation9. Once the presumpti-ve diagnosis of atrial myxoma has been made prompt surgical resection is the best option because of the risks of serious complications like embolization or sudden death. Preoperative coronary angiography is indicated in selected patients (coronary artery disease suspected, age over 40 years, etc.) to assess the coro-nary arteries10. Postoperative recovery is usually good. However, early complications can occur. Supraventri-cular arrhythmias (premature heart beats, short-las-ting atrial fibrillation), atrio-ventricular blocks, pne-umonia, pleural effusion, wound infection have been described11,12.
Postoperative early and late mortality ranges from 0 to 7.5%12,13. Damaged valve may require repair or re-placement, but it was not necessary in this case. One month after discharge the anterior mitral valve was thickened possibly due to chronic tumoral injury, with moderate regurgitation and slight pulmonary hyper-tension (the right ventricle to an atrium gradient of 29 mmHg) (Figure 7). Three months after the operation the patient is recovered with no signs of recurrence. The prognosis in our patient is good, but follow-up is necessary because of the risk of recurrence which can be as high as 13%14,15.
The particularity of this case is the high impact given by the tumor obstruction of the left ventricle inflow, resulting in very poor exercise capacity with chronic exertional dyspnea which was initially considered to be due to hypothyroidism.
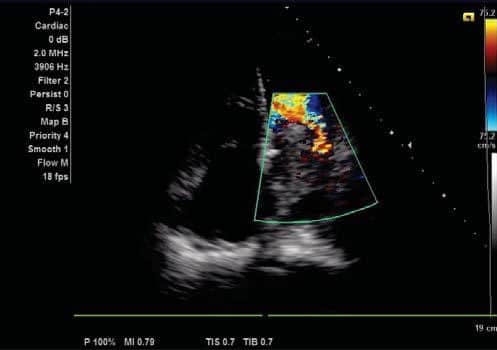
Figure 3. Apical 4 cambers. Left atrial tumor and mitral regurgitation.

Figure 4. Post-operative view of the tumor.
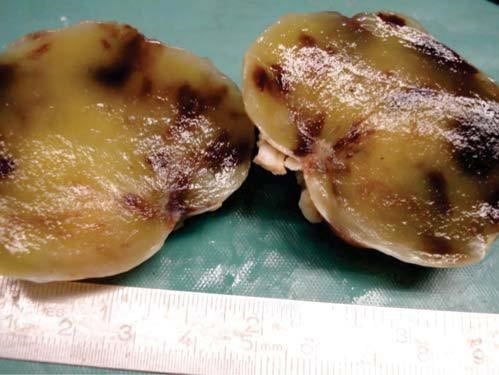
Figure 5. Macroscopic view of myxoma. The tumor is very well delimited, oval-shaped, elastic consistency, smooth surface and brownish yellow with purplish areas color.
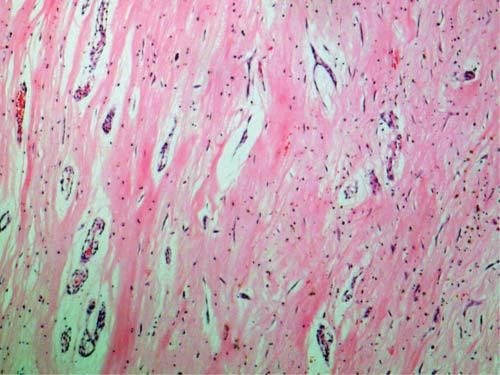
Figure 6. Photomicrograph of myxoma. The fragment is represented by a mixoid tissue which consist of elongated cells with reduced paled eo-sinophilic cytoplasm and hyperchromatic nuclei. The cells are disposed in groups and rows. The mixoid stroma consists of liniar deposits of calcium and iron (Gandy-Gamna bodies) and reduced lymphocytic infl amatory in-filtrate (Hematoxylin and eosin).
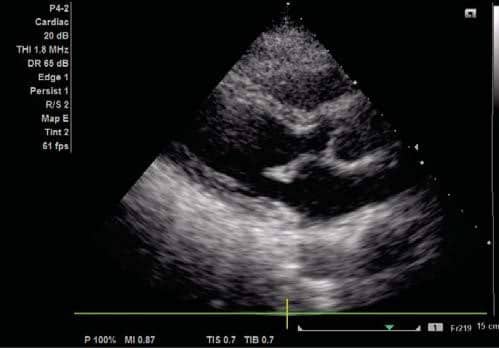
Figure 7. Parasternal long axis.
CONCLUSIONS
In summary, cardiac myxomas are rare condition in clinical practice. High index of suspicion is mandato-ry for diagnosis and prompt therapy. Urgent surgical resection is indicated because of the high risk of com-plications and of sudden death, with low procedural mortality and morbidity.
Conflict of interest: none declared.
References
1. Abraham KP, Reddy V, Gattuso P. Neoplasms metastatic to the heart: review of 3314 consecutive autopsies. Am J Cardiovasc Pathol. 1990; 3: 195–198
2. Yu K, Liu Y, Wang H, Hu S, Long C. Epidemiological and pathological characteristics of cardiac tumors: a clinical study of 242 cases. Inter-act Cardiovasc Thorac Surg. 2007 Oct:6(5):636-9.
3. Bjessmo S, Ivert T. Cardiac myxoma: 40 years’ experience in 63 pa-tients. Ann Thorac Surg. 1997;63:697–700
4. Ermek T, Aybek N, Zhang WM, Guo YZ, Guo S, Mamataly A, Chang DQ, Liu J, Zhang ZG. A rare case of biventricular myxoma. J Cardio-thorac Surg. 2017 Mar 27;12(1):17. doi: 10.1186/s13019-017-0584-6.
5. Sabzi F, Nasiri B. Myxoma of the Superior Vena Cava Origin Present-ed as a Right Atrial Mass. J Teh Univ Heart Ctr 2013;8(4):202-204.
6. Karimi VM, Anushiravani A, Dabbaghmanesh MH, Hosseinzadeh M, Rasekhi AR, Zamirian M, Anushiravani A. Myxoma Immediately above the Junction of the Inferior Vena Cava and the Right Atrium: A Rare Cause of Budd-Chiari Syndrome. J Tehran Heart Cent. 2016 Jul 6;11(3):139-142.
7. Ramphal PS, Spencer HW, Mitchell DI, Denbow CJ. Myxoma of right femoral vein origin presenting as a right atrial mass with syncope. Thorac Cardiovasc Surg. 1998 Oct;116(4):655-6.
8. Larrieu AJ, Jamieson WR, Tyers GF, Burr LH, Munro AI, Miyagishima RT, Gerein AN, Allen P. Primary cardiac tumors: experience with 25 cases. J Thorac Cardiovasc Surg. 1982 Mar;83(3):339-48.
9. Johnson TR, Becker CR, Wintersperger BJ, Herzog P, Lenhard MS, Reiser MF. Images in cardiovascular medicine. Detection of cardiac metastasis by positron-emission tomography-computed tomog-raphy. Circulation. 2005 Jul 26;112(4):e61-2.
10. Dumitrasciuc G, Gaspar M, Ionac A, Jusca C, Deutsch P, Petres-cu L, Mut-Vitcu B, Stefan I. Dragulescu SI. Left atrial myxoma as-sociated with coronary artery disease – uncommon challenge. TMJ 2004:54(4): 370-73
11. Lee KS, Kim GS, Jung Y, Jeong IS, Na KJ, Oh BS, Ahn BH, Oh SG. Sur-gical resection of cardiac myxoma-a 30-year single institutional ex-perience. J Cardiothorac Surg. 2017 Mar 27;12(1):18. doi: 10.1186/ s13019-017-0583-7.
12. Perek B, Misterski M, Stefaniak S, Ligowski M, Puślecki M, Jemielity M. Early and long-term outcome of surgery for cardiac myxoma: experi-ence of a single cardiac surgical centre. Kardiol Pol. 2011;69(6):558-64.
13 Keeling IM, Oberwalder P, Anelli-Monti M, Schuchlenz H, Demel U, Tilz GP, Rehak P, Rigler B. Cardiac myxomas: 24 years of experi-ence in 49 patients. Eur J Cardiothorac Surg. 2002 Dec;22(6):971-7.
14. Iliescu VA, Dorobantu LF, Stiru O, Iosifescu AG, Coman I, Marin S, Filipescu D. A doua recidiva a unui mixom cardiac aparuta la 7 ani de la prima operatie. Chirurgia. 2008:103(2): 239-241.
15. Elbardissi AW, Dearani JA, Daly RC, Mullany CJ, Orszulak TA, Puga FJ, Schaff HV. Survival after resection of primary cardiac tumors: a 48-year experience. Circulation. 2008 Sep 30;118(14 Suppl):S7-15.
 This work is licensed under a
This work is licensed under a