Maria Dorobanţu1, Daniela Bartoş2, E. Apetrei3, Cătălina Arsenescu-Georgescu4, Dana Pop5, S. Ghiorghe2, Rodica Tănăsescu6, Elvira Craiu7, I. Maniţiu8, Oana Tăutu1
1 ”Carol Davila” University of Medicine and Pharmacy – Clinical Emergency Hospital Bucharest, Cardiology Department
2 ”Carol Davila” University of Medicine and Pharmacy – Clinical Emergency Hospital Bucharest, Internal Medicine Department
3 ”Carol Davila” University of Medicine and Pharmacy, “Prof. Dr. C. C. Iliescu” Institute of Cardiovascular Diseases Bucharest, Cardiology Department
4 “Gr.T. Popa” University of Medicine and Pharmacy, “Prof. Dr. George I. M. Georgescu” Institute of Cardiovascular Diseases Iasi, Medical Cardiology Department
5 ”Iuliu Hatieganu” University of Medicine and Pharmacy – Clinical Recovery Hospital Cluj-Napoca, Clinical Cardiovascular Recovery Department
6 CMI Dr. Rodica Tanasescu, Bucharest
7 Ovidius University Constanta – General Medicine Faculty, Clinical Emergency County Hospital Constanta, Cardiology Department
8 “Lucian Blaga” University Sibiu – “Victor Papilian” Faculty of Medicine, Emergency County Hospital Sibiu, Cardiology Department
Prof. Dr. Maria DOROBANŢU, Head of Cardiology Department, Clinical Emergency Hospital Bucharest, Calea Floreasca no. 8, sector 1, postal code 014461, Bucharest. Phone: 004021-5992264. Fax: 004021-3170108.
E-mail: maria.dorobantu@gmail.com
Abstract: Objectives – To evaluate prevalence, treatment and control of hypertension in Romania in 2012 and to find targets for developing prevention strategies aiming at improving hypertension management in Romania. Methods – SEPHAR II is a national representative cross-sectional survey with previous described aims. Thus, between October 2011 – March 2012 (2 study visits), 1975 subjects aged between 18 and 80 years, 52.6% women were evaluated through a questionnaire (socio-demographic data, risk factors and historical medical) blood pressure measurements and laboratory tests. The response rate was 69%. Results – The prevalence of hypertension is 40.1%, increasing with age and is higher in women than in men only in rural areas. Although more than half (59.1%) of hypertensive patients are treated, of which 72.7% are treated with two or more antihypertensive drugs, blood pressure control was noted in only 25% of those treated. Conclusion – The current prevalence of hypertension is still high and despite the improvement in awareness and treatment, control of hypertension remains a daunting challenge. Middle age hypertensive subjects from rural areas, with low level of education, low average income and without medical insurance represent the target for future interventions aimed to improve hypertension management in Romania.
Keywords: hypertension, prevalence, treatment, control, national, survey
Abstract: Obiective – Evaluarea prevalenţei, tratamentului şi controlului hipertensiunii arteriale în România, în 2012 şi identificarea ţintelor pentru dezvoltarea unor strategii de îmbunătăţire a managementului hipertensiunii arteriale în România. Metode – SEPHAR II este un studiu naţional transversal desfăşurat pe un eşantion reprezentativ pentru populaţia României având obiectivele enunţate. Astfel, între octombrie 2011 – martie 2012 (2 vizite de studiu), 1975 subiecţi cu vârste între 18 şi 80 de ani, 52,6% femei, au fost evaluaţi prin intermediul unui chestionar (date socio-demografice, factori de risc şi istoric medical) măsurarea tensiunii arteriale şi analize de laborator. Rata de răspuns a fost de 69%. Rezultate – Prevalenţa hipertensiunii este 40,1%, crescând odată cu vârsta, fiind mai mare la femei decât la bărbaţi numai în zonele rurale. Deşi peste jumătate (59,1%) dintre pacienţii hipertensivi sunt trataţi, dintre care 72,7% sunt trataţi cu 2 sau mai multe antihipertensive, controlul tensiunii arteriale a fost consemnat doar la 25% din cei trataţi. Concluzie – Prevalenţa actuală a hipertensiunii arteriale în
România este încă ridicată şi, în ciuda îmbunătăţirea gradului de conştientizare şi de tratament, controlul hipertensiunii arteriale rămâne provocarea descurajantă. Hipertensivii de vârstă mijlocie, din mediul rural, cu nivel scăzut de educaţie, venituri mici şi fără asigurare medicală reprezintă ţintele viitoarelor intervenţii menite să îmbunătăţească managementul hipertensiunii arteriale în România.
Cuvinte cheie: hipertensiune arterială, prevalență, tratament, control, național, supraviețuire
INTRODUCTION
From the health policy planning perspective it is very important to know the prevalence of lifestyle-dependent cardiovascular disease risk factors. Even more importantly, policy planners should be aware of trends regarding the prevalence of CVD risk factors in the population. This would allow them to anticipate future trends in mortality, and evaluate the benefits of various population-based prevention strategies concerning cardiovascular diseases.
Until SEPHAR project initiation in 2005, the available data on hypertension (HT) prevalence in Romania were from studies conducted on selected populations showing a variable HT prevalence (depending on the type of studied population) and therefore without being representative for the entire population1-4.
SEPHAR I was the first epidemiologic study conducted on a representative sampling for the entire country population and whose results can outline the general direction of prevention programs. Its results confirmed Romania as a high cardiovascular risk country2,5-8.
After 2006, three other major epidemiological studies were conducted in Romania regarding cardiovascular risk factors but on selected populations (general practitioners’ patients, patients with ischemic heart disease or patients of certain departments of cardiology) do not allow extrapolation of the results to the entire population of Romania2,9-11.
SEPHAR I’s unicity lays in the fact that so far it is the only epidemiologic survey with a follow-up of 7 years through SEPHAR II survey.
The main objective of this paper is to evaluate prevalence, treatment and control of hypertension in Romania in 2012 and to find targets for developing prevention strategies aiming to improve hypertension management in Romania, as revealed by the two SEPHAR surveys.
METHODS
The methodology of SEPHAR II survey was broadly similar to SEPHAR I that has been previously described5-7. Briefly it is a cross-sectional national survey conducted on a representative sample for the Romanian Adult population (obtained by means of proportional multi-stratified sampling) in which subjects of both sexes aged between 18 to 80 years were evaluated by trained general practitioners (GPs) in 2 study visits 7 to 10 days apart. The study was approved by the local ethics committee and all the enrolled subjects gave written informed consent to participate.
The sampling procedure and the criteria used in this procedure are the same ones as in SEPHAR I survey (teritorial regions: Romania’s area was divided in 8 regions: North-Est (NE: Bacău, Botoşani, Iaşi, Neamţ, Suceava, Vaslui), South-East (SE: Brăila, Buzău, Constanţa, Galaţi, Tulcea, Vrancea), South (S: Argeş, Călăraşi, Dâmboviţa, Giurgiu, Ialomiţa, Prahova, Teleorman), South-West (SW: Dolj, Gorj, Mehedinti, Olt, Vâlcea), West (W: Arad, Caraş-Severin, Hunedoara, Timiş) North-West (NW: Bihor, Bistriţa-Năsăud, Cluj, Maramureş, Satu-Mare, Sălaj), Central region (Alba, Braşov, Covasna, Harghita, Mureş, Sibiu) and Bucharest region (Bucharest and Ilfov), based on the National Statistics Institute’s recommendations which takes into account health indices also), locality type (cities with over 200 000 inhabitants, cities with 50 000-200 000 inhabitants, cities with less than 50 000 inhabitants and communes), gender and age groups (18-24 years, 25-34 years, 35-44 years, 45-54 years, 55-64 years and 65-80 years)5-7.
For a research population of 16.833.541 adult people (calculated based on Population and Housing Census from 18th -27th March 2002 provided by the National Institute of Statistics) of which 40.1% are estimated to be hypertensive (according to SEPHAR I results8), with a maximum error of ± 2.18% at a confidence level of 95%, the minimum required sample size is: 1942 subjects.
The number of subjects needed to be included from each sampling stratum (teritorial regions, locality type, gender and age group) in the final sample was calculated so that the weight of stratum subjects in the final sample is equal to the weight of stratum population in the whole Romanian adult population.
In order to comply with the low Law number 677/2001 for the protection of individuals with regard to processing of personal data and the free movement of such data we selected individual addresses corresponding to subjects with a specific demographic charactetistics (a certain age group, a ceratin sex, from a certain locality) from the database of Romanian Population General Direction of Data Records in which addresses are listed alphabetically by street name using a selection step defined by the ratio between the total population from a certain locality and the number of subjects needeed to be included in the final sample from that locality. The starding point on the list (the first selected adress) was defined by devideing by 2 the selection step. Trying to overcome the difficulties in finalising a case, the number of selected addresses was the double of the number of needed subjects except for Bucharest region where the number of selected addresses was the triple.
At each study visit 3 blood pressure (BP) measurements were done with at least 1 minute between them, according to current recommendations12,13 (in seated position after at least 5 minutes rest with their backs supported and previously advised not to smoke or drink coffee within 30 minutes prior to the assessment, after adjusting the cuff size to the arm circumference: standard cuff if arm’s circumference is <32cm and large cuff if the arm’s circumference is ≥32 cm) using an automatic oscillometric BP measuring device – model A&D UA 95 Plus certified by Association for the Advancement of Medical Instrumentation (AAMI). Prior to the 3 measurements, BP was measured at each arm and then the 3 measurements were made at the arm with the highest value.
The visit BP value was the average of the second and third measurement from each of the 2 study visits (without taking into account the first BP measurement from each visit).
Hypertension (HT) was defined as systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg at both study visits or previously diagnosed HT under treatment during the last two weeks, regardless of BP values.
Awareness of HT was defined by the percent of hypertensive subjects who declared being previously diagnosed with HT by a medical professional.
Severity of HT was assessed only in newly diagnosed subjects according to the ESH/ESC guidelines (mild HT: SBP between 140-159 mmHg and/or DBP between 90-99 mmHg; moderate HT: SBP between 160-169 mmHg and/or DBP between 100-109 mmHg and severe HT: SBP ≥180 mmHg and/or DBP ≥110 mmHg) taking into account the maximum value of the two mean SBP/DBP values from each study visits. If the severity of arterial HT according to the SBP value was different from that according to the DBP value, the worse one was taken into account.
BP control was defined as SBP less than 140mmHg and DBP less than 90 mmHg in treated hypertensive patients13.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics 20.0 software at a significance level of p <0,05 by a company specialized in medical research.
A descriptive analysis (means, medians, standard deviations and range for continuous data and frequency analysis for categorical data) was performed for all target variables.
Kolmogorov-Smirnov test was used to analyze continuous data distribution, according to which appropriate tests were further used in analysis: independent samples t-test or Mann-Whitney U test for differences between means of 2 independent groups, ANOVA or Kruskal-Wallis test for differences between means of ≥3 independent groups. Chi-square test was used to analyze differences between categorical data.
The statistical significance of differences between results of SEPHAR II and SEPHAR I was assessed using binomial test for categorical data and one-sample t-test for continuous data.
RESULTS AND DISCUSSIONS
SEPHAR II response rate (RR)
Between October 15th 2011 and March 15th 2012 a total number of 2860 addresses from 182 study sites were visited by the study investigators approaching a total 2223 subjects (637 subjects not found at the address) from which only 1975 subjects had eligible data for the analysis (complete questionnaires + both study visits) (179 subjects denied participation and 69 were excluded as follows: 28 subjects with protocol violation (age above 80 years), 36 subjects incomplete study, 2 subjects protocol violation (age above 80 years) and incomplete study and 3 missing case report forms), leading to a 69,06% RR, value that is significantly higher than SEPHAR I’s RR5 (69,06% vs. 44,26%; p <0.0001).
The total sample of 1975 subjects with eligible data for analysis satisfies the sample size criteria for representativity.
General prevalence of hypertension in Romania
Of all respondents (1975 subjects), on the basis of the above-mentioned criterion, the presence of HT was recorded in 40.4% of cases (798 subjects), in majority representing a previously known condition (newly diagnosed hypertension (ndHT) – 243 cases, 12 3% vs. known hypertension (kHT) – 555 cases, 28.1%,
p <0.0001).
Thus, we can estimate – with an error of ± 2.2% at a confidence level of 95% that currently in our country there are about 7 millions hypertensive adults (6.800.751. hypertensive adults from the total 16,833,541 romanian adults) of which about 5 millions are known hypertensives (4.730.225) and about 2 millions were diagnosed during SEPHAR II survey (2.070.526).
Compared with the situation 7 years ago, the general prevalence of HT in Romania has significantly decreased by 10.7% together with the reduction to almost half in the prevalence of newly diagnosed HT while the prevalence of known HT has increased by 41.3% (Table 1).
Table 1. Global prevalence of HT by regions in SEPHAR surveys
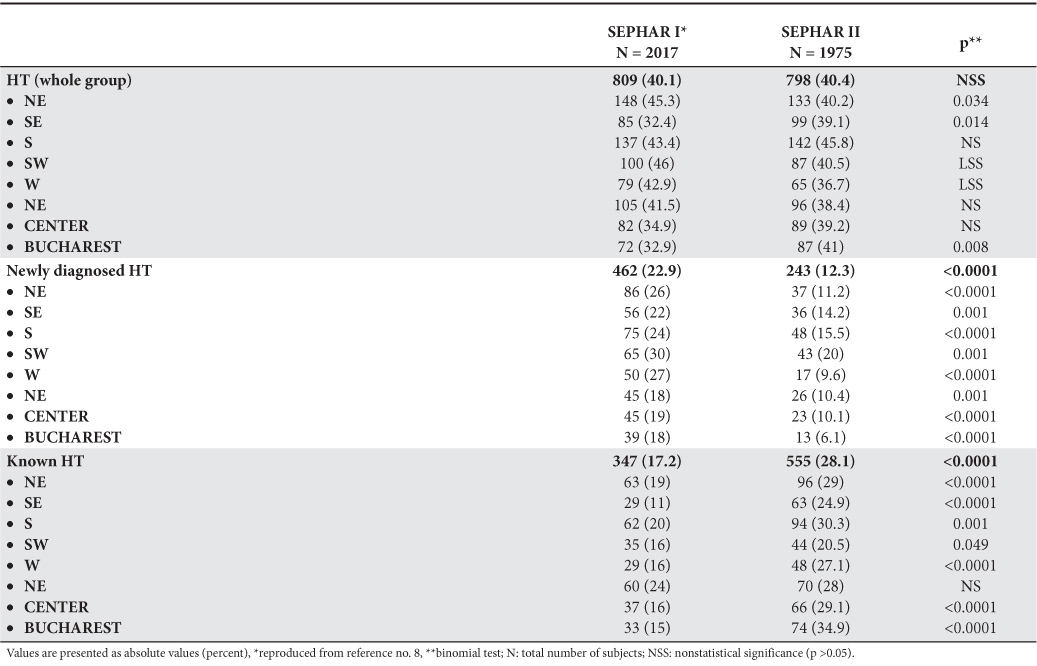
Prevalence of HT by teritorial regions
The highest prevalence of hypertension was recorded in the South region, the proportion of hypertensive subjects recorded in this region was statistically significantly higher than those recorded in the other 7 regions [NE: 40.2% vs. SE: 39.1% vs. S: 45.8% vs. SV: 40.5% vs. V: 36.7% vs. NV: 38.4% vs. Center: 39.2% vs. Bucharest: 41% vs. 40.4%; p <0.0001].
Except for South-West region, where the proportion of known hypertensives was statistically similar to that of newly diagnosed hypertensive [newly diagnosed hypertension – 20% vs. known hypertension – 20.5%; p = 0.915] in the other 7 regions, the proportion of known hypertensive subjects was statistically significantly higher than that of newly diagnosed hypertensive subjects [NE: ndHT – 11.2% vs. kHT – 29%, p <0.0001, SE: ndHT – 14.2% vs. kHT – 24.9%, p = 0.007, S: ndHT – 15.5% vs. kHT – 30.3%, p <0.0001; W: ndHT – 9.6% vs. kHT – 27.1%, p <0.0001; NW: ndHT – 10.4% vs. kHT – 28%, χ2 = 20.167, p <0.0001; Center: ndHT – 10.1% vs. kHT – 29.1%, χ2 = 20.775, p <0.0001; Bucharest: ndHT – 6.1% vs. kHT – 34.9%, χ2 = 47.770, p <0.0001], similar to the situation observed for the entire group.
The largest proportion of newly diagnosed HT was recorded in the South-West region [NE: 11.2% vs. SE: 14.2% vs. S: 15.5% vs. SW: 20% vs. W: 9.6% vs. NW: 10.4% vs.. Center: 10.1% vs. Bucharest: 6.1% vs. 40.4%, p <0.0001], and the highest proportion of known hypertension was recorded in Bucharest region [NE: 29% vs. SE: 24.9% vs. S: 30.3% vs. SW: 20.5% vs. W: 27.1% vs. NW: 28% vs. Center: 29.1% vs. Bucharest: 34.9%, p <0.0001].
Analysis of prevalence of hypertension in the 8 regions showed statistically similar values to those observed for the entire group except for South region where the recorded prevalence of hypertension was significantly higher than that recorded in the whole group [NE: 40.2% vs. 40,4%, p = 0491, SE: 39.1% vs. 40.4%, p = 0.366, S: 45.8% vs. 40.4%, p = 0.030; SW: 40.5% vs. 40.4%, p = 0.518, W: 36.7% vs. 40.4%, p = 0.179, NW: 38.4% vs. 40.4%, p = 0.282; Center: 39.2% vs. 40.4%,
p = 0.384; Bucharest: 41% vs. 40.4%, p = 0451].
Compared with SEPHAR I survey’s results regarding the prevalence of HT across the 8 teritorial regions there is an increase in prevalence of HT in the South-East and Bucharest regions, a decrease in prevalence of HT in the North-East, West and South-West regions (for the last 2 regions, the difference between the two surveys has borderline statistical significance), a significant decrease in the proportion of newly diagnosed HT together with an increase in the proportion of known HT, in all 8 regions (the difference in proportions of known HT for North-West region hasn’t reached statistical significance) (Table 1).
Prevalence of HT by age groups
As expected, the prevalence of HT increased with age, the highest prevalence being recorded in the ≥65 years age group (18-24 years – 11, 1% vs. 25-34 years – 7.8% vs. 35-44 years – 23.1% vs. 45-54 years – 49.7% vs. 55-64 years – 65.8% vs. ≥65 years – 81%, p <0.0001), increase that is independent of patient’s sex and area of residence.
The highest prevalence of newly diagnosed HT was recorded in the 45-54 years age group (18-24 years – 8.9% vs. 25-34 years – 6% vs. 35-44 years – 11.4% vs. 45-54 years – 17.1% vs. 55-64 years – 15.1% vs. ≥65 years – 14%, p <0.0001) while the highest prevalence of known HT was recorded in the ≥65 years age group (18-24 years – 2.2% vs. 25-34 years – 1.8% vs. 35-44 years – 11.7% vs. 45-54 years – 36.2% vs. 55-64 years – 50.7% vs. ≥65 years – 67%, p <0.0001).
The differences observed between the 6 age groups in both prevalence of newly diagnosed HT and known HT are independent of sex and area of residence.
Compared with SEPHAR I survey’s results there has been no change in HT prevalence among the youngest group and among both the 45-54 years and 55-64 years groups, while a significant decrease has been noticed in the both 25-34 years and 34-44 years groups (by 47.66% and by 17.92% respectively) and a significant increase in the oldest group (by 7.91%) (Table 2).
Table 2. HT prevalence by age, sex and area of residence across SEPHAR surveys
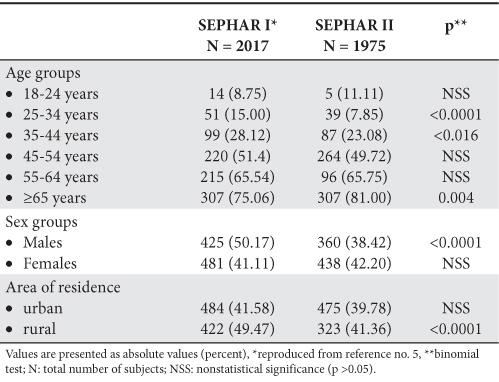
Prevalence of HT by gender
Hypertension prevalence among female (F) subjects is significantly higher than that of males (M) subjects only in rural areas (F: 40.6% vs. M: 36%, p = 0.003), while in urban areas HT’s prevalence is similar in both genders (F: 41.1% vs. M: 39.5%, p = 0.831).
Similarly, gender differences regarding both the prevalence of newly diagnosed HT and known HT were noticed only in rural areas where males had significatly higher prevalence of newly diagnosed HT than females (F: 13.9% vs. M: 19.9%, p = 0.025) who instead had a significantly higher prevalence of kHT (F: 32.7% vs. M: 16.1%; p <0.0001).
In the last seven years, HT prevalence has decreased by 23.42% among adult male population, while in female adult population it has remained the same (Table 2).
Prevalence of HT by areas of residence
While the general prevalence HT recorded in rural and urban areas were similar (rural – 41.4% vs. urban – 39.8%, p = 0.486), the prevalence of newly diagnosed HT recorded in rural areas was statistically significantly higher than that recorded in urban ones [rural – 16.9% vs. urban – 9.3%, p <0.0001) where instead the prevalence of known HT is significantly higher (rural – 24.5% vs. urban – 30.5%, p = 0.004).
Compared with SEPHAR I survey’s results, there has been a 16.39% decrease of HT prevalence in rural areas, while in urban ones it has remain the same (Table 2).
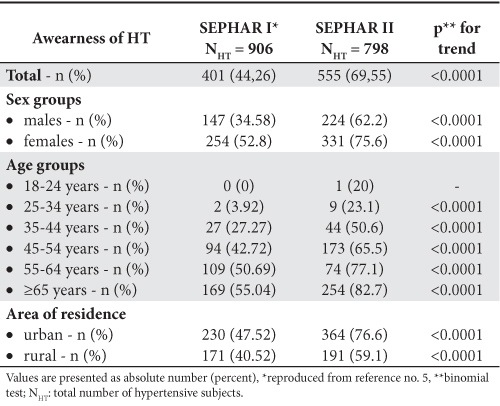
Awareness of HT
From the total 798 hypertensive subjects, 555 subjects (69,5%) were aweare of their condition. The level of awareness increased with age (18-24 years: 20% vs. 25-34 years: 23.1% vs. 35-44 years: 50,6% vs. 45-54 years: 65.5% vs. 55-64 years: 77.1% vs. ≥65 years: 82.7%;
p <0.0001) regardless of the gender, and it was higher in medically insured subjects (uninsured: 29,6% vs. insured: 73.3%, p <0.0001) and in females than in males only in rural area (F: 129 cases, 70.1% vs. M: 62 cases, 44.6%; p <0.0001) and with no sex differences in urban areas (F: 202 cases, 79.5% vs. M: 162 cases, 73.3%; p = 0.110).
Since 2005 the level of awareness of HT has significantly and consistently increased in both genders, all age groups and both areas of residence (Table 3).
Table 3. Awareness of HT across SEPHAR surveys
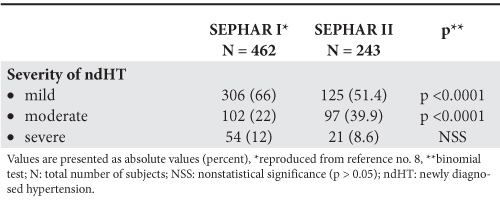
Severity of newly diagnosed HT
In terms of severity, about half of newly diagnosed hypertensive subjects had BP values corresponding to mild hypertension (mild HT: 51.4% vs. moderate HT: 39.9% vs. severe HT 8.6%, p <0.0001).
There were no significant differences regarding the severity of newly diagnosed HT by age, gender, territorial regions or area of residence.
Compared with the situation 7 years ago, there was a significant decrease in the proportion of mild HT cases and a significant increase in the proportion of moderate HT cases while the proportion of severe HT cases was similar in the two surveys (Table 4).
Table 4. Severity of newly diagnosed HT across SEPHAR surveys
Hypertension treatment and control
From the total 798 hypertensive subjects, current antihypertensive treatment was recorded in 472 of them representing 85% of the known HT subjects and 59.1% of all hypertensive subjects.
Females were more frequently treated than males regardless of their place of living. Medically insured hypertensives are more frequently treated than those uninsured, regardless of their gender (Table 5).
Table 5. HT treatment across SEPHAR surveys
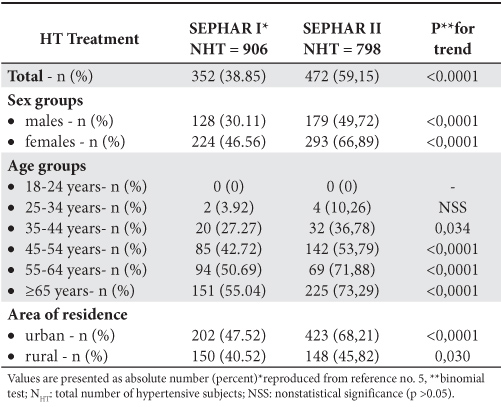
There were significant differences regarding the proportion of treated hypertensives across the 8 territorial regions increasing from the smallest value of 42.5% recorded in the South-West region to up to the highest value of 79.3% recorded in Bucharest region. Treatment of HT was significantly more frequently recorded in urban than in rural ones only in North-East, South-East, South-West and Bucharest region, while in the other 4 regions there was no significant difference between rural and urban regions.
The majority of treated hypertensives were using 2 or more antihypertensive drugs (1 drug: 27.3% vs. 2 drugs: 39.6% vs. 3 or more drugs: 33.1%; p = 0.005), the maximum recorded number of antihypertensive drugs used being 5.
The two most used antihypertensive drugs were ACE inhibitors (59.1%) and diuretics (58.9%) in similar proportions, followed by beta-blockers (53.2%). The large proportion of patients in whom beta-blockers were used could be explained by the prevalence of ischemic heart disease and heart failure in our adult population (10.2% for ischemic heart disease and 4.2% for heart failure) conditions in which beta-blocker treatment has class I A indication.
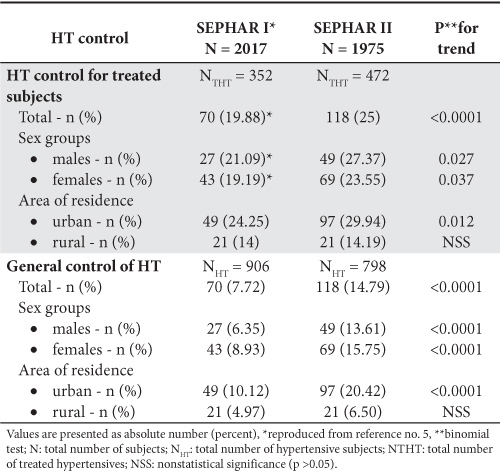
An effective treatment (BP <140/90 mmHg) was recorded in only 118 subjects representing 25% of the total treated hypertensives and 14.8% of all hypertensive subjects.
The therapeutic control rate ranged between the lowest value of 11.3%, recorded in the SE region, up to the higest value of 39.1%, recorded in Bucharest region, and was higher in urban areas than in rural ones but without gender or medical insurance status differences. An important finding was the increase in the therapeutic control rate both with the increase of educational level (the therapeutic control rate in subjects with higher education is double than that of uneducated subjects) and the increase in average income per person (hypertensive subjects with controlled BP values had a significantly higher average income per person than subjects without treatment control).
These results were explained by the fact that treatment control depended more on subject’s adherence to treatment, importantly influenced by the level of education. More, people with higher education tended to have a job, and thus to have a better income than subjects with lower levels of education and in this way they had a better access to antihypertensive drugs and thus a higher treatment control rate.
Changes in HT treatment and control recorded in the last seven years consisted in a significant increase in the proportion of treated hypertensives, the decrease in use of monotherapy together with the increase in use of 3 or more antihypertensive drugs. ARBs, antihypertensive agents that were not available in our country 7 years ago, are currently used by 16.7% of treated hypertensives. As a result of these changes in treatment the general BP control rate has doubled in both genders only in urban areas, whereas in rural ones general BP control rate was the same as 7 years ago (Table 5).
Out of the 354 treated hypertensive subjects without controlled BP values, 27.7% were receiving 3 or more antihypertensive drugs out of which one was a diuretic and therefore being considered as having resistant to treatment HT.
We cannot estimate the true prevalence of resistant hypertension in our adult population based on the findings of this study, due to the fact that de definition used to classify subjects as having resistant HT does not rule out all the possible causes of a false resistant HT such as poor treatment adherence or other causes of secondary HT.
Table 6. BP control across SEPHAR surveys
Where are we?
Summarizing all the above results, we could conclude that in 2012 we are on a descending trend regarding HT prevalence and on an upward trend regarding HT’s awarenss, treatment and control. But despite these encouraging results, we are a country where HT’s prevalence is still high and BP control represents still a doubtfull challenge.
Currently, we have only a rough estimate of the magnitude of resistant hypertension in Romania based on the SEPHAR II survey’s results which showed that 27.7% of all treated hypertensives who had BP values ≥140/90 mmHg were under current treatment with at least 3 including a diuretic. This assessment can not exclude the many causes of false resistance to treatment. Therefore we can estimate that the true prevalence of resistant hypertension in Romania has a value lower than 27.7%, in the worst case scenario representing a quarter of treated and uncontrolled hypertensives.
At european level, even though Romania seems to align together with some Central European countries such as Czech Republic and Poland regarding HT’s prevalence and awareness14,15, regarding HT’s treatment and especially BP control it lays together with the other Balkan countries, probably due to economic reasons16-21.
What can we do?
In the light of the SEPHAR II survey’s results, which proved to be a useful epidemiologic tool, continuing with annually follow-up by means of a simple questionnaire completed with laboratory-work-up at every 5 years seems a natural way to continue monitoring the changes in HT’s prevalence and management.
The results of SEHAR II survey showing a rough estimate of the prevalence of resistant HT in Romania highlights the crucial importance of a National Registry of Resistant HT which is currently unavailable. The development of such a registry is a step forward that must be made by all healthcare authorities.
The focus of future interventions should be on middle age hypertensive subjects from rural areas with low level of education, low average income and without medical insurance in order to achieve a better BP control and thus a significant decrease in cardiovascular mortality in our country.
Acknowledgement:
The first author (Maria Dorobanțu) and the last author (Oana-Florentina Tăutu) have equal contribution to this paper.
The authors express their gratitude to those who brought their contribution to the SEPHAR II study: Dr. Tomas Zdrojewski from Poland, for support regarding methodology development and for logistic support, Servier Pharma Romania, for financial and logistic support during the whole study duration, Clar Research SRL for the support regarding sampling, data management and statistical analysis of the data and last but not least to all the general practitioners, nurses and residents that have been involved in this study (Appendix 1).
Conflict of interests: None disclaimers.
This study was realized with financial support from Romanian Society of Hypertension and from SERVIER PHARMA – Romanian Branch.
References
1. Ginghină C., Popescu B., Şerban M. et al. The Prevalence of hypertension and left ventricular hypertrophy in a Romanian population. A clinical – echocardiographic study. J. Hypertens, 2004; 22, suppl 2: S307.
2. Dorobanțu M., Tăutu O. Proiecte româneşti de cercetare a factorilor de risc cardiovascular. Medicina Interna, 2012; IX, suppl 2012: 7-14.
3. Apetrei E., Kulcsar I., Stănescu Cioroianu R. şi col. Studiul Urziceni – Studiu populaţional prospectiv de depistare a factorilor de risc pentru bolile cardiovasculare şi intervenţie în populaţie, depistartea precoce a bolilor cardiovasculare. Revista Română de Cardiologie, 2008; vol XXIII, Nr. 2: 136-145.
4. Apetrei E., Kulcsar I., Stănescu Cioroianu R. şi col. Studiul Urziceni – Studiu populaţional prospectiv de depistare a factorilor de risc pentru bolile cardiovasculare şi intervenţie în populaţie, depistartea precoce a bolilor cardiovasculare. Revista Română de Cardiologie, 2008; vol XXIII, Nr. 4: 305-316.
5. Dorobanţu M, Darabonţ RO, Bădilă E, and Ghiorghe S. Prevalence, Awareness, Treatment, and Control of Hypertension in Romania: Results of the SEPHAR Study. Int J Hypertens., 2010; doi:10.4061/2010/ 970694.
6. Dorobanţu M, Bădilă E,Ghiorghe S, Darabonţ R.O, Olteanu M and Flondor P. Total Cardiovascular Risk Estimation in Romania. Data from SEPHAR Study. Rom J Intern Med. 2008;46(1):29-37.
7. Dorobanţu M, Darabonţ RO, Bădilă E. et al. SEPHAR study – Study for Evaluation of Prevalence of Hypertension and cardiovascular risk in adult population in Romania – Part I: Methodology. Romanian Heart Journal. 2006; vol XXI; 2: 89-96.
8. Dorobanţu M, Darabonţ RO, Bădilă E. et al. SEPHAR study – Study for Evaluation of Prevalence of Hypertension and cardiovascular risk in adult population in Romania – Part II: Results. Romanian Heart Journal. 2006; vol XXI; 3: 179-190.
9. Cinteză M., Pană B., Cochino E. et al. Prevalence and control of cardiovascular risk factors in Romania cardio-zone national study; Maedica – A Journal of Clinical Medicine, 2007; Vol. 2, Nr. 4: 277-288.
10. Macarie C., Chioncel O., Ionescu D.D., Căpâlneanu R. Studiul ”Angina treatment pattern” (ATP) în România. Premize, rezultate şi comparaţii. Medicina Internă, 2008; 1.
11. Matei C., Pop I., Jurcuţ R. et al. Romanian Multicentric Study of the Prevalence of Metabolic Syndrome – ROMES, Hellenic Journal of Cardiology, 2008: 49: 303-309
12. Mancia G, De Backer G, Dominiczak A. et al. 2007 Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2007;25:1105–1187.
13. Mancia G, Laurent S, Agabiti-Rosei E, et al. Reappraisal of European guidelines on hypertension management: a European Society of Hypertension Task Force document. J Hypertens 2009; 27: 2121–58.
14. Cífková R, Skodová Z, Bruthans J. et al. Longitudinal trends in cardiovascular mortality and blood pressure levels, prevalence, awareness, treatment, and control of hypertension in the Czech population from 1985 to 2007/2008. J Hypertens. 2010 Nov; 28(11):2196-203.
15. Zdrojewski T, Szpakowski P, Bandosz P. et. Al. Arterial hypertension in Poland in 2002. J Hum Hypertens. 2004 Aug;18(8):557-62.
16. Vera G, Nataša D, Svetlana K. et. al. Epidemiology of hypertension in Serbia: results of a National Survey. J E Epidemiol. 2012;22(3): 261-6. Epub 2012 Feb 25.
17. Jelaković B, Dika Z, Kos J. et al. Treatment and control of hypertension in Croatia. The BEL-AH study. Lijec Vjesn. 2006 Nov-Dec; 128(11-12):329-33.
18. Accetto R. Arterial hypertension as a public health issue in Slovenia. Blood Press Suppl. 2005 Dec;2:22-4.
19. Efstratopoulos A.D., Voyaki S.M., Baltas A.A. et.al. Prevalence, awareness, treatment and control of hypertension in Hellas, Greece: the Hypertension Study in General Practice in Hellas (HYPERTENSHELL) national study. Am J Hypertens. 2006 Jan;19(1):53-60.
20. Altun B, Arici M, Nergizoğlu G. et al. Prevalence, awareness, treatment and control of hypertension in Turkey (the PatenT study) in 2003. J Hypertens. 2005 Oct;23 (10):1817-23.
21. Sonkodi B, Sonkodi S, Steiner S. et al. High prevalence of prehypertension and hypertension in a working population in Hungary. Am J Hypertens. 2012 Feb;25(2):204-8. doi: 10.1038/ajh.2011.199.
Appendix 1.
SEPHAR II survey’s investigators:
Afrim Valentin, Andrei Mirela, Balauta Lucia, Bostan Elisabeta, Bratosin Remus, Bunescu Florin, Caliman Marinela, Cantaragiu Daniela, Chelarescu Costilena, Chirlejan Carmen, Cioloboc Iulia, Cirin Horia, Ciusleanu Ruxandra, Clinic Maria, Coman Mihaela, Cordea Delia Cosmeleata Ion, Cucoanes Cristina, Culda Ligia, Culicianu Doru, Curetean Raluca, Dascal Pompilia, Dogaru Adriana, Doniga Milena, Dragne Carmen, Dulipovici Milena, Dumitrescu Dragos, Dumitrescu Ileana, Ene Aqueline Karina, Faragau Adriana, Florescu Dan, Florescu Mirela, Gavrilescu Dan, Gheberta Nicoleta, Gheorghiu- Tudor Titina, Grecu Cristinel, Grigoriu Adina, Guzga Cristina, Hudici Virgiliu Daniel, Ionescu Viorica, Ionica Carmen Silvia, Iordache Cleopatra, Isac Doina, Lakatos Maria, Lascu Gheorghe, Marinescu Anca, Micu Draga, Mihaila Carmen, Moaca Adriana, Mosneaga Daniela Ligia, Motoran Daniela, Muresan Sofia, Neagoe Daniela, Neagu Laura, Nedelcu Daniela, Nistor Cristina, Nistor Ileana, Olaru Diana, Oltean Violeta, Olvedi Iosif, Deaconu Daniela Florina, Orbocea Daniel Victor, Palade Emilian, Papuc Ruminita, Parvan Doru, Pasztor Gyongyver, Peia Andreia, Petrache Angelica, Petrescu Amalia, Priscoveanu Angela, Radoiu Anina, Rusti Anca Valentina, Sarbu Elena, Sarbu Teodora, Sipos Elisabeta, Sosdeanu Marius, Spanoiu Mihai, Tamasoi Monica, Taraboante Anca-Paula, Tatucu Cristian, Tite Dorina, Tofan Alexandru, Tolnai Angela, Toma Ioana Daciana, Tomescu Viorel Dan, Topologeanu Gabriela, Trifescu Daniela, Tudorache Elena, Udrea Dumitra, Ulita Andreea, Ungureanu Mihai, Ungurianu Daniela, Uta Leonard, Varlan Constantin, Viisoreanu Melania, Vladimirescu Suzana, Vlas Smaranda, Vleju Victoria, Vonica Roxana Georgeana, Zarnoianu Zizi, Zbarcea Silvia, Tranca Iulia,
Residents involed in the SEPHAR II survey:
Dragoescu Bogdan, Marinescu Mihai, Vacarescu Cristina, Onciul Sebastian, Bataila Vlad, Deaconu Alexandru, Comanescu Ioana, Georgescu Alina, Rotaru Iulia, Udrea Florian, Micoara Adolf, Borga Ciprian, Silea Daniela, Iana Andreea, Costea Andreea Codrina, Nagy Elena, Florea Ramona, Andrei Razvan, Lupu Dragos, Codrut Ciurea, Zah Anamaria, Mada Laura, Marginean Teodora, Laslo Ioana, Natrapazu Alina, Iosip Adriana, Markovits Corina, Sabiescu Bogdan Mihai, Adrian Raducan, Damian Iulia, Vasile Roxana, Popescu Monica, Batar Sergiu, Bolea Florina, Teodoru Minodora, Mirica Daniel.
 This work is licensed under a
This work is licensed under a