Antoniu Petriş1, Gabriel Tatu-Chiţoiu2, Călin Pop3
Article received on the 11th of February 2013. Article accepted on the 6th of March 2013.
1 University of Medicine and Pharmacy “Grigore T. Popa”, “Sf. Spiridon” Emergency Hospital, Cardiology Clinic, Iaşi
2 Emergency Hospital “Floreasca”, Department of Cardiology, Bucureşti
3 County Emergency Hospital Baia Mare, University “Vasile Goldiş”, Arad, Romania
Antoniu Petriş, MD, University of Medicine and Pharmacy “Grigore T. Popa”, “Sf. Spiridon” Emergency Hospital, Cardiology Clinic, B-dul Independenţei nr. 1 Iaşi 700111 antoniupetris@yahoo.com
Abstract: Background – The quality of physicians’ private lives is responsible for maintaining an optimal quality level of their professional lives. Objective – Evaluating the quality of Romanian cardiologists’ private lives by self-rating their happiness degree, health and involvement in managerial/social/volunteer/religious activities, as well as the ways they choose to spend their free-time in. Method – Members of Romanian Society of Cardiology (RSC) were invited to respond to a confidential on-line questionnaire available over a 30 day period. Results – A group of 187 cardiologists participated: age 45.69±9.78 years, experience in the field of 13.95±8.70 years; 75 (40%) male; 109 (58.28%) consultants; 55 (29.41%), specialist registrars and 23 (12.29%) junior doctors; 135 (72.19%) were general cardiologists, while 35 (18.71%) were interventional/ intensivists. Quality-of-live happiness-degree and health self-rating were scaled 1 (most pessimistic evaluation) to 5 (most optimistic evaluation). The average scores were 3.34±0.92 and 3.94±0.74, respectively. As far as the quality-of-life was concerned, men scored higher than women (3.52±0.89 vs 3.21±0.92 p = 0.026), cardiologists performing abroad scored higher than the ones performing exclusively into Romania (4.00±0.73 vs 3.90±0.74 p = 0.033), and married scored higher than single ones (p=0.010). Almost 13% of respondents were smokers, 38% overweight / obese, 76.47% do not spend their free-time doing outdoors activities, and more than 33% practice no sports whatsoever. The quality-of-life rating score of the happiest cardiologists was directly correlated to their professional level: junior doctors / specialist registrars / consultants (p<0.01) and years of activity in cardiology (p = 0.035). Conclusions – 1. A high percentage of cardiologists are smokers, overweight / obese, do not spend their free-time doing outdoor activities and do no sports. 2. Cardiologists least happy are young, single, had previously worked abroad, do not work in the academic environment, have less than 21 paid vacation days a year, do not own personal households, and are neither interventional cardiologists, nor emergency cardiology physicians. 3. These data can be a milestone for the education of Romanian cardiologists in cardiovascular disease prevention offering an initial reference point for rating their further outcome. 4. These data can also be used by the RSC among arguments of improving Romanian cardiologists’ quality-of-life in front of decision makers of the national health system.
Key words: cardiologist, lifestyle, happiness, questionnaire, quality-of-life
Introduction
Happiness can be defined as “a state of intense and absolute contentment” (approximate translation from DEX – The Explanatory Dictionary of the Romanian Language)1. Quality-of-life evaluations measure the dependency between living conditions and individual perceptions, states of mind, satisfaction or lack of it, happiness or frustration2,3. Considering the major impact that private life has over the professional one, the quality of physicians’ private lives is more and more subject to such evaluations. Giving the context, we asked ourselves how happy / content Romanian cardiologists really are. Using a model recently tested in the United States of America4 as its parting point, the present survey aims to provide you with an answer to the very question, being the first of its kind ever to be conducted in Romania.
Aims
The aim of present survey was to evaluate the quality-of-life of Romanian cardiologists by means of a questionnaire allowing them to self-rate degrees of private life happiness and health.
Methods
The survey was initiated and coordinated by the Acute Cardiac Care Working Group of the Romanian Society of Cardiology (SRC), and was grounded on an on-line questionnaire (docs.google.com) representing an adaptation of the toll used by US physicians to self-rate their happiness/contentment degree (MEDSCAPE “Physician lifestyle Report”)4. The American questionnaire was published in January 2012 and contains answers provided by 29025 physicians representing 25 medical fields, 762 of the respondents being cardiologists. In spite of our persistent efforts, we were unable to identify other similar evaluations thus data filled in by Romanian cardiologists were compared exclusively to data in the American survey. The list of questions is available in Table 1. A 5 point score was used in order for the sample to self-rate the quality of their private lives, where 1= “least happy” and 5 = “happiest”). Same way, another 5 point score was used for the self-rating of the physical health, where 1=”least healthy” and 5 = “healthiest”). Members of Romanian Society of Cardiology were asked to answer the questionnaire between September 1st and 30th, 2012 and a single recall was performed during this interval. Preliminary data were communicated at the “Cardiovascular prevention: a national emergency” Session of the National Congress of Cardiology (October 4th-6th, 2012).
Table 1. Questionnaire rating Romanian cardiologists’ quality-of-life – components
Ethical considerations: The questionnaire was confidential; a format enabling respondents to fill in their answers under protection of anonymity was used (docs.google.com). Moreover, Romanian Society of Cardiology transmitted an official commitment to confidentiality to all its members. Legal provisions in the field – Law No. 677/2001 on the Protection of Individuals with Regard to the Processing of Personal Data and the Free Movement of Such Data, amended and completed, and Law No. 506/2004 on the processing of personal data and the protection of privacy in the electronic communications sector – were respected accordingly.
Statistical analysis: Data collected were centralized in an Excel data base (Microsoft ® Office Excel 2003) and analyzed using a specialized software (SPSS 14.0; SPSS, Chicago, Illinois). Results are presented as average ± standard deviation (SD). Student’s T-Test was used to compare the independent continuous variables, while chi test2 was used to compare proportions. A value of p <0.05 was considered statistically significant.
Results
General data: One hundred eighty-seven colleagues, 45.69±9.78 years old (range 27 to 74 years old, median 45), with an activity in cardiology of 13.95±8.70 years (1 to 47 years, median 13) answered the questionnaire. Seventy-five (40.11%) were male, and 112 (59.89%) female. More than half – 109 (58.29%) – were consultants (“primari”) in cardiology, 55 (29.41%) were specialist registrars (“specialiști“), and 23 (12.28%) were junior doctors (“rezidenți”) from which 2.12% were in their 1st to 3rd year of residency, and 10.16% were in their 4th to 5th year of residency. Most of the respondents, i.e. 135 (72.19%) were general cardiologists, 22 (11.76%) were interventional cardiologists, 13 (6.95%) were cardiologists working in Coronary Care Units, 6 (3.21%) were cardiovascular rehabilitation specialists, 2 (1.07%) were pediatric cardiologists, and 9 (4.81%) had a different area of activity. One hundred and five respondents (56.15%) performed academic activities. More than two thirds of the respondents (103; 69.52%) were working both in public hospitals, and in private clinics; 37 (19.79%) were working only in public hospitals, while 20 (10.70%) were working in the private sector exclusively. Thirty-eight (20.32%) of the total number of respondents had worked abroad for certain time periods, while 110 (58.82%) stated their availability to seizing such opportunity.
One hundred and forty-one respondents (75.40%) were married, 9 (4.81%) were remarried, 13 (6.95%) were divorced, 3 (1.60%) were widowers and 21 (11.23%) were single. In 82 cases (43.85%) married respondents’ life partners were also physicians, in 13 cases (6.95%) they were involved in activities related to medical care, and in 71 cases (38.97%) they had non-medical professions. The average number of children was 1.21±0.90 (0 to 4 children, a median of 2). Most participants (147; 78.61%) declared themselves as being religious individuals although non-practicants, 33 (17.65%) affirmed being religious and practicants, while 7 (3.74%) were atheists.
Financial status: Ninety-eight respondents (52.41%) live in personal block apartments, 75 (40.11%) own houses, 14 (7.49%) live in rented households. Most respondents (159; 85.03%) own a car. Most of the respondents (116, 64.09%) declared no financial debts, while 12 (6.63%) reported debts lower than EUR 5000, 36 (19.89%) reported debts between EUR 5000 and 50 000, and 17 (9.39%) reported debt amounts exceeding EUR 50 000.
Cardiovascular risk factors: Cardiovascular risk factors distribution as reported by respondents is presented in Figure 1:
– Smoking/Non-smoking: Two thirds of the respondents (118; 63.10%) were non-smoking, 47 (25.13%) used to smoke but quit, while 24 (12.83%) were active smokers.
– Hypertension. A number of 29 respondents (15.51%) were diagnosed with hypertension.
– Dyslipidemia. Almost one third of the respondents reported suffering from lipid disorders (57; 30.48%).
– Diabetes: Three colleagues (1.60%) mentioned themselves as having diabetes.
– Overweight / Obesity: Only one hundred sixty-two from the total 187 respondents mentioned their Body Mass Index (BMI). Five respondents (3.09%) declared a BMI under 18.4 kg/m2 (underweight), 95 respondents (58.64%) between 18.5 and 24.9 kg/m2 (normal weight), 49 respondents (30.25%) between 25 and 29.9 kg/m2 (overweight), and 13 respondents (8.02%) declared a BMI over 30 kg/m2 (obese).
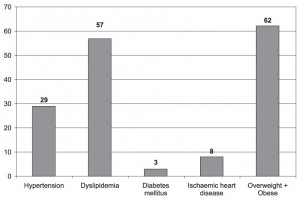
Figure 1. Cardiovascular risk factors distribution (no. of respondents).
Physical exercise: One third of the respondents (68; 36.36%) reported they exercise 30 minutes a day. Twenty-two of our colleagues (11.76%) reported doing physical exercises for one hour every day, 8 (4.28%) reported doing physical exercises for two/more hours daily, while 47 (25.13%) admitted exercising only weekly (Figure 2). Forty-two (22.46%) of the respondents declared no daily exercising at all. One hundred eighteen (63.10%) of our colleagues reported practicing at least one sport. A top 5 most frequent sports includes: 1. Gymnastics/Aerobics/Tai Chi (44; 23.53%); 2. Swimming (41; 21.93%); 3. Skiing (29; 15.51%); 4. Cycling (24; 12.83%); 5. Athletics (17; 9.09%). Other mentioned sports were: tennis (12; 6.42%), table tennis (9; 4.81%), basketball (6; 3.21%), football (5; 2.67%), volleyball (3; 1.60%), climbing (1; 0.53%), martial arts (1; 0.53%). Twelve respondents (6.42%) participated in local sports competitions, 3 (1.60%) in national competitions and one colleague (0.53%) was engaged in international competitions. One third of the respondents (69 colleagues, 36.90%) declared practicing no sports whatsoever.
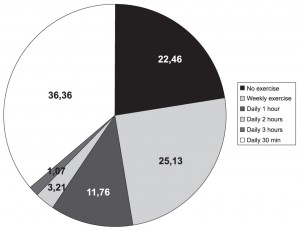
Figure 2. Sample distribution according to physical exercise frequency.
Free-time activities: Most of the respondents (101; 54.01%) mentioned having 21 to 29 vacation days a year, 60 (32.09%) mentioned 14 to 20 days, 18 (19.63%) mentioned over 30 days, and 8 (4.28%) mentioned only 7 to 13 vacation days yearly. The number of days spent on vacation was positively correlated to the quality-of-life rating score (r=0.195, p <0.01). The favorite vacation is spent either in Romania, or abroad (118; 63.10%), and is mentioned clearly most frequently than vacations spend exclusively abroad (60 respondents; 32.09%) or only in Romania (9; 4.81%). The majority of the respondents (126 respondents, 67.38%) prefer both sea-side and mountains as vacation destinations, 36 respondents (19.25%) choose mountains exclusively, while 25 of them (13.37%) choose only the sea-side. Outdoor recreation is appreciated by only 49 respondents (hunting: 3, i.e. 1.60%; fishing: 14, i.e. 7.49%; camping 32, i.e. 17.11%), while for the most of them (143; 76.47%) spending free-time in the middle of the nature is not a preferable free-time activity. Main ways for spending free-time are: 1. traveling (135; 72.19%); 2. reading (127; 67.91%); 3. movie watching (94; 50.27%); 4. visiting friends (93; 49.73%); 5. shopping (70; 37.43%). Physical exercise barely holds the 7th position amongst Romanian cardiologists’ preferences (n=63; 33.69%).
Only 54 respondents (28.9%) admitted owning social networking accounts. The lack of interest (or of available time !) for joining social networking is also characteristic to American cardiologists who hold top position among the 25 medical specialties inquired who declare a low use of such social connection methods.
Alcohol consumption: Twenty-three respondents (12.30%) declared no alcohol consumption whatsoever, 139 (74.33%) declared consuming alcohol occasionally, 24 (12.83%) mentioned moderate consumption, and one respondent (0.53%) mentioned high alcohol consumption. Only 18 respondents (9.63%) prefer beer, 56 (29.95%) have opted for wine, and 8 (4.28%) for spirits consumption.
Community life involvement: A number of 63 respondents (33.69%) declared managerial involvement (hospital manager, head of department, private managing), 8 (4.28%) declared political involvement, 54 (28.88%) declared social involvement (sponsorships, arts patronage, donations), and 54 (28.88%) declared volunteer-type involvement (pro-bono activity, tutoring, counseling, international/religious missions).
Quality-of-life happiness degree: The evaluation of the happiness degree concerning the quality-of-private life was scored 1 to 5 points as described in the methodology of the survey (Figure 3).
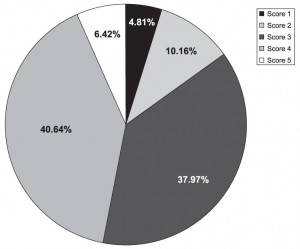
Figure 3. Sample distribution considering answers provided to the question: “Are you happy with your private life?” (1 to 5 point score).
The average score was 3.34±0.92, lower than the value of 3.92 (no standard deviation indications available) reported in the American questionnaire3 (Figure 4).
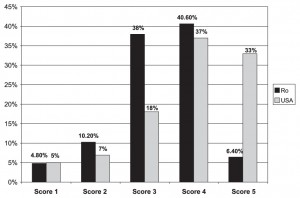
Figure 4. Romanian vs American quality-of-life rating scores distribution – comparison (see reference 3).
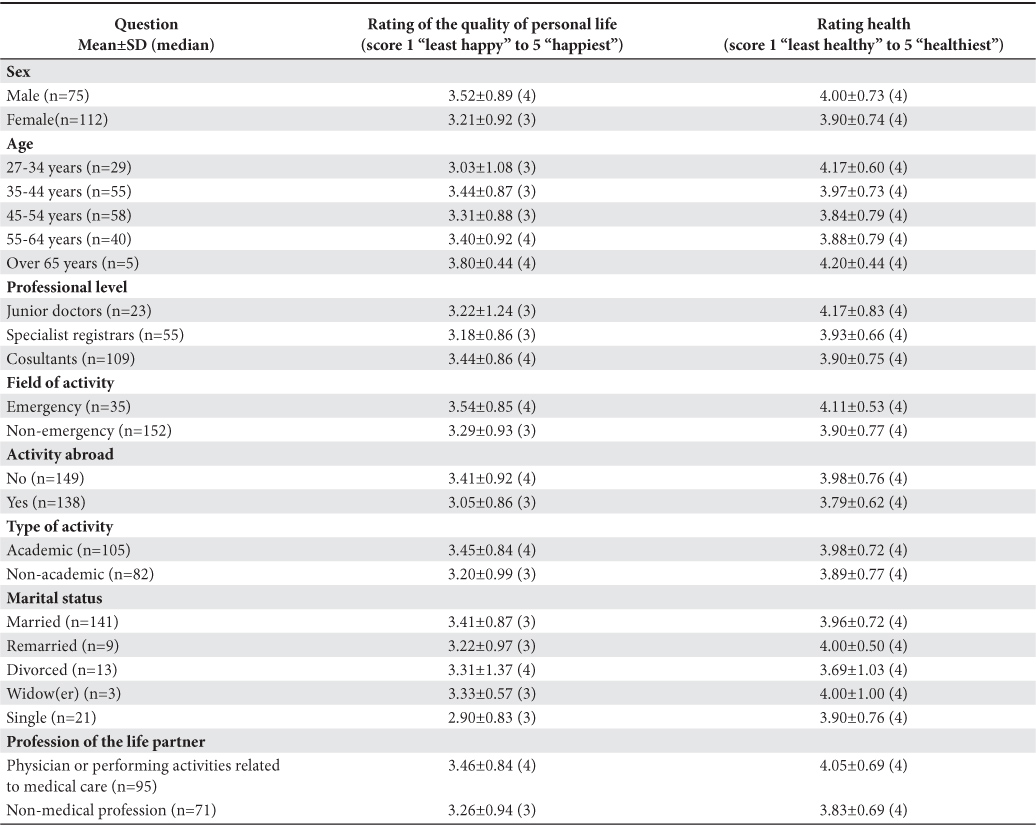
Average happiness degree was higher in males (3.52±0.89, median 4) as opposed to females (3.21±0.92, median 3) (p=0.026). Highest quality-of-life average score was registered in respondents age over 65 (3.80±0.44), followed by the sub-groups ages 35 to 44 (3.44±0.87) and 27 to 34 (3.03±1.08), still no statistically significant differences were identified except group age 27 to 34 vs group age 55 to 64 (p=0.049). Consultants were the happiest (3.44±0.86), followed by specialist registrars (3.22±1.24) and junior doctors (3.18±0.86), but the differences were not statistically significant. Interventional cardiologists and intensivists registered an insignificant higher score (4.11±0.53) than physicians not working in these areas (3.54±0.85) (p=0.143). An interesting detail, i.e. average quality-of-life score in cardiologists who previously worked abroad was lower (3.41±0.92) than the one of their colleagues working within national borders exclusively (3.98±0.76, p =0.033). No statistical differences were registered between the scores of respondents performing in the academic environment as opposed to the ones not doing so (3.45±0.84 and respectively 3.89±0.77, p=0,063), nor between consultants and specialist registrars (3.44±0.86 vs 3.18±0.86, p=0.072) or between junior doctors and specialist registrars / consultants (3.22±1.24 vs 3.44±0.86 / 3.18±0.86, p=0.508); statistical differences also failed to appear when comparing married to single cardiologists (3.41±0.87, and 2.90±0.83, respectively; p = 0.010), and respondents whose life-partners were either physicians or persons involved in activities related to medical care to respondents whose life-partners were working in non-medical fields (3.46±0.84 vs 3.26±0.94, p = 0.155) (Table 2).
Table 2. Quality-of-life and health rating scores in different categories of respondents
Quality-of-life versus life-length: The majority of the respondents (146; 78.07%) mentioned quality-of-life and life-length as being equally important; for 37 respondents (19.79%) the quality-of- life is more important than its duration, while for one colleague (0.53%) life-length is the most important of the two. Three respondents (1.60%) checked the “I don’t know / I haven’t yet thought about it” box in the questionnaire. The best way to prolong one’s lifetime is considered to be the aggressive care regime by 47 of the respondents (25.13%), the palliative care by 27 respondents (14.44%) or the ceasing of any drug administration by 11 respondents (5.88%); still, the majority (102; 54.55%) checked the “I don’t know / I haven’t yet thought about it” box.
Self-rating health: Average health self-rating score was 3.94±0.74 (Figure 5), lower than the average of 4.17% reported by American cardiologists4.
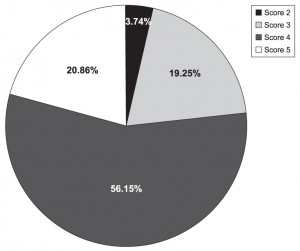
Figure 5. Sample distribution considering health self-rating (1 to 5 point score).
Cardiologists who previously worked abroad considered themselves less healthy (average index = 3.05±0.86) than the ones working exclusively in Romania (3.79±0.62) (p=0.033). No significant differences were registered between males vs females (4.00±0.73, and 3.90±0.74, respectively), between junior doctors (4.17±0.83) and specialist registrars (3.90±0.75)(p=0.123), or between interventional cardiologists / intensivists (3.90±0.77) and respondents not working in these areas (3.29±0.93)(p=0.143); significant differences also failed to appear when comparing respondents performing in the academic environment (3.98±0.72) to the ones not doing so (3.89±0.77) (p=0.063), and also when comparing respondents whose life-partners were either physicians or performing activities related to medical care (4.05±0.69) to respondents whose life-partners were working in non-medical fields (3.83±0.69)(p=0.155). Higher health self-rating scores were reported by young respondents (27 to 34 years old) (4.17±0.60) and respondents age over 65 (4.20±0.44), yet no statistically significant difference was identified.
Happiest versus least happy respondents – comparison:
When comparing data reported by the least happy cardiologists (quality-of-life rating scores 1+2) to data reported by the happiest cardiologists (scores 4+5) (see Table 3), respondents least happy (n=28) are significantly younger (42.25±10.28 years vs 46.73±9.75 years, p=0.039), single (21.43% vs 5.68% married, p=0.046), work less frequent in emergency cardiology (10.71% vs 22.72%, p<0.001) and own in a significantly lower percentage personal households (25.00% vs 52.27%, p=0.001), but consider themselves healthier (average index = 4.22±0.63 versus 3.36±0.73, p<0.001). The least happy respondents had worked abroad (25% versus 13.64%) or would prefer to work abroad (82.14% versus 51.14%). Moreover, the least happy are more, yet insignificantly, frequently married to life-partners working in non-medical fields than to life-partners working in the medical field (46.43% versus 32.95%, p=0.059), have more frequently (yet no statistically significant) financial debts exceeding EUR 50 000 (14.29% vs 9.09% cardiologists with lower debts, p=0.082), or automobiles (71.43% vs 92.05%, p=0.077).
Table 3. “Least happy” respondents (score 1+2) versus “happiest” respondents (score 4+5) – comparison
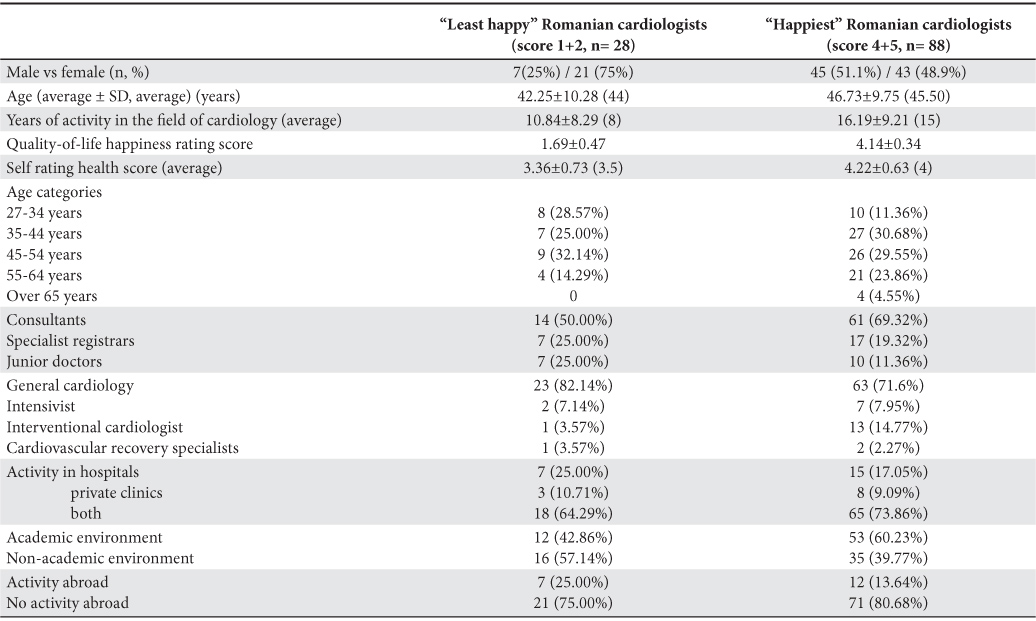
The percentage of the happy ones was higher in case of colleagues performing in the academic environment (60.23% versus 42.86%). The difference was not, however, significant, probably due to the relative low number of respondents (p = 0.109).
Respondents having a BMI over 30 kg/m2 (overweight/obese) appeared more frequently as happy with the quality of their lives (40.3%) as compared to the least happy ones (28%). Furthermore, happiest respondents have more vacation days a year (over 21 days) (71.6% vs 46.4%, p=0.008), are more frequently religious practicants (14.77% vs 7.14%, p=0.005), are less abstinent when considering alcohol (9.09% vs 28.57%, p=0.009), prefer in an slightly more frequent consumers of beer (11.4% vs 3.6%, p=0.224) and wine (34.1% vs 21,4%, p=0.211) and declare a managerial, political, social or volunteer involvement similar to the one mentioned by the least or less happy (22.73% vs 21.43%, p=0.119; 5.68% vs 3.57%, p=0.664, 32.95% vs 25%, p=0.432 and respectively, 29.55% vs 25%, p=0.646).
Apparently the most satisfied with the quality of personal life prefer to spend their vacations abroad (34,1% vs 17,9%, p=0.650) and in the mountains (28.6% vs 19.3%, p=0.678); exercise more frequent 30 minutes / day (42% vs 35.7%, p=0.895) and participate more frequent in local sports competitions (9.1% vs 3.6%, p=0.683); still, when it comes to outdoor recreation activities this category scores 75% vs 82.1%, p=0.440 and also reports lower interest in social networks (23.9% vs 35.7%, p=0.221). This absolutely differences did not appear statistically significant due probably to the relatively low number of respondents.
Quality-of-life rating score declared by the happiest cardiologists was correlated to their professional level (p<0.01) and the years of activity in the field of cardiology (p=0.035).
The least happy cardiologists see the problem of the best treatment to be applied for prolonging lifetime the same way their happiest colleagues do, i.e. aggressive care: 25% vs 28.41%, p=0.348; palliative care: 14.29% vs 15.91%, p=0.468, but the option for ceasing all drug administration is more frequently reported by the happiest (5.68% vs 3.57%, p=0.001). No significant differences were registered between the two subgroups from the point of view of the incidence of hypertension, diabetes, dyslipidemia or ischemic heart disease (17.9% vs 14.8%, p=0.698; 7.1% vs 1.1%, p=0.082; 28.6% vs 27.3%, p=0.895; 7.1% vs 3.4%, p=0.401).
Discussions
The present questionnaire rating physicians’ health and happiness degree concerning their quality-of-life is the first of its kind ever to be conducted in Romania. For comparison purposes, we insistently, yet unsuccessfully, tried to identify specific data reported in other European countries. Basically, the one and only source we could compare our data to was the American questionnaire4 published in January 2012, which was used as a model for our questionnaire. Our purpose was not that of creating to a syndicalist questionnaire, although some of our colleagues might have expected it to be so. Our analysis revealed a series of particularities of Romanian cardiologists, some of them being really surprising. Thus, almost 13% of Romanian cardiologists are smokers (and 25% are ex-smokers). By comparison, only 1% of American cardiologists smoke4. Over 38% of respondents were either overweight (30%) or obese (8%). More than one third of the cardiologists do not do sports. Only 19% of them mentioned daily exercise, 36% report moderate 30 minute daily physical activity, while 25% dedicate only weekends to doing sports. More than three quarters of respondents do not spend their free-time outdoors, within nature, preferring traveling, reading, movie watching, visiting friends or shopping as alternatives. By comparison, 70% of American cardiologists prefer to spend their free-time in doing physical activities4.
Quality-of-life happiness index of Romanian cardiologists (3.34+0.92) was inferior to the value reported by American cardiologists (3.92). In fact, considering all 25 medical specialties participating to the American questionnaire, the happiest respondents were the rheumatologists (score = 4.09), followed by dermatologists (score = 4.06) and urologists (score = 4.04), while the least happy were the internists (score = 3.88), gastroenterologists (score = 3.88) and neurologists (score = 3.88). American cardiologists (762 respondents)4 came 15th. By comparison to these data, the average quality-of-life rating score provided by Romanian cardiologists places them under the level reported by any of the 25 specialties who responded to the American questionnaire.
Least happy with the quality of their lives are the young cardiologists, cardiologists having less de 21 paid vacation days a year, colleagues who previously worked abroad, colleagues not performing in the academic environment, the ones not owning personal households, those who are single and, interesting, cardiologists not working in emergency in interventional cardiology. Still, the least happy ones have lower BMIs and higher health indexes when compared to the group of the happiest. Cardiologists age over 65, consultants in cardiology, intensivists and the ones who never worked abroad are the happiest ones. The overall health index of Romanian cardiologists is relatively high (3.94) but lower than the one reported by American cardiologists (4.17)4.
An aspect we find important to be highlighted is that a number of 141 respondents to our questionnaire (75.40%) were married, a percentage lower than the one reported by American cardiologists (81.2%). The rate of divorced (and not remarried) cardiologists was higher in case of Romanian cardiologists (6.95% vs 5.5%). This aspect is significantly important, as divorce rate reported by American cardiologists was found by MEDSCAPE to be higher than the average of 3.3% registered at the level of all analyzed specialties4. Family life is an extremely important reference point also highlighted by our survey; the difference between average quality-of-life rating scores was statistically significant when comparing single cardiologists to married ones (p=0.010).
Over 95% of the respondents consider themselves religious individuals. By comparison, 85% of MEDSCAPE 2012 respondents declared themselves as such4. Moreover, WIN-Gallup International’s recent poll, i.e. “The Global Index of Religiosity and Atheism” placed Romanians on 6th position in the international top of most religious peoples worldwide (89%)6.
One could ask themselves why such data about professional groups, Romanian cardiologists in our case, are relevant to be collected and reported. We believe quantifiable data are needed considering the relation of interdependency between the quality of one’s private life and their professional performances7. Such data are the only means for evaluating the “Work Life Balance” concept and help ourselves, in a context in which contemporary organizations became “greedy” for employees’ time8, especially for the time of the highly specialized ones, amongst who cardiologists are to be found. These series of introspections become even more relevant in the context of Romania belonging together with Latvia and Lithuania to the group of countries where the overall average of life-happiness decreased on the background of severe recession9. According to some sources, lowest happiness levels are registered by Romania and Hungary – EU member states, followed by Armenia and Georgia – two Caucasian countries9.
As a consequence, we believe this first Romanian cardiologist’ quality-of-life rating to be valuable from at least three points of view: 1. The survey highlights a set of particularities that should alarm part of the cardiologists (the relatively high number of smokers, overweight/obese colleagues, as well as that of cardiologists not doing constant physical exercise). Mentioned particularities must become as many targets hunted down by Romanian Society of Cardiology in its efforts to prevent cardiovascular diseases; 2. Data collected lay the perfect grounds for comparison as far as evaluating immediate future evolutions in our specialty is concerned; 3. Present data can be included in the set of arguments we present to health policy decision makers in support of our efforts to improve Romanian cardiologist’s quality-of-life. Such efforts should represent a constant concern for all our fellow cardiologists.
Study limitations
The apparent main limitation of the present survey is the low number of respondents, only 187 (approximately 19% of the total number of Romanian cardiologists). Nevertheless, we believe this group to represent a significant sample as far as our specialty is concerned, considering the proportional distribution revealed (58% consultants, 24% specialist registrars, 12% junior doctors) which corresponds to the national proportional distribution of mentioned professional categories. By comparison, the American questionnaire was answered by a little over 700 cardiologists, such total being most probably inferior to the percentage of Romanian respondents if taking into account that the entire US population is 14 times grater than the one of Romania10.
Conclusions
1. The scores of the cardiologists’ happiness degree concerning their quality-of-life and the health self rating one were 3.94±0.74 and 3.34±0.92, respectively. Both scores were lower compared with the ones reported in the American questionnaire.
2. A high percentage of cardiologists are smokers (12.83%), overweight /obese (38%), do not enjoy outdoor activities as a way of spending their free-time (76.47%), and practice no sports whatsoever (over 33%).
3. Least happy with the quality of their lives are the young cardiologists, cardiologists having less than 21 paid vacation days a year, those who previously worked abroad, those not performing in the academic environment, single ones, those not owning households, and those not working in the emergency cardiology field or in that of interventional cardiology. The least happy cardiologists have a lower BMI and consider themselves healthier than the ones happy or happiest with the quality of their lives.
4. Data revealed by our analysis lay the grounds for the development of educational activities in the field of cardiovascular disease prevention conducted by Romanian Society of Cardiology; such concern should evidently extend more and more among its members. Information collected are useful for evaluating future evolution of the efforts made in the field of educating prevention and can easily be included in the set of valid arguments used by Romanian Society of Cardiology in front of sanitary policy decision makers in support of our plea for improving the quality-of-life of the Romanian cardiologists.
Acknowledgements
The authors are grateful to Daniela Petriş for her skillful assistance and continued support and to Anca Tatu-Chițoiu for the English translation of this text.
Conflict of interest: none declared.
References
1. Academia Română. Institutul de Lingvistica “Iorgu Iordan”. Dictionarul explicativ al limbii române DEX. Ed. Univers Enciclopedic Gold, Bucureşti, 2012.
2. Mărginean I. Calitatea vieţii în România: prezent şi perspective. Calitatea Vieţii 2010; 3–4: 231–237.
3. West CP, Shanafelt TD. Physician well-being and professionalism. Minn Med. 2007; 90: 44-46.
4. Peckham C. Profiles in happiness: which physicians enjoy life most? http://www.medscape.com/features/slideshow/lifestyle/2012/cardiology
5. Wood S. Cardiologists Are Happy(ish), Married Non-Tweeters, Survey Reveals. Medscape. Mar 22, 2012. http://www.medscape.com/viewarticle/760775
6. WIN-Gallup International. The Global Index of Religiosity and Atheism 2012. Win Gallup International, Washington DC, 2012.
7. West CP, Shanafelt TD, Kolars JC. Quality of Life, Burnout, Educational Debt, and Medical Knowledge Among Internal Medicine Residents. JAMA. 2011; 306: 952-960.
8. Ivan GA. Echilibrul dintre muncă şi viaţa personală în România. Cauze, efecte şi tendinţe. Teza de doctorat 2011 http://www.unibuc.ro/studies/Doctorate2011Noiembrie/Ivan%20Georgiana%20Aurelia%20-%20Echilibrul%20dintre%20munca%20si%20viata%20personala%20in%20Romania/rezumat.pdf
9. European Bank for Reconstruction and Development. The Life in Transition. After the crisis. 2011. www.ebrd.com/lifeintransition
10. Institutul Naţional de Statistică. Romania în cifre 2012. Ed. Revista Română de Statistică, Bucureşti, 2012.
 This work is licensed under a
This work is licensed under a