Lelia Strimbu1,2, Ioana Dregoesc1, Radu Hagiu1
1 “Niculae Stancioiu” Heart Institute, Cluj-Napoca, Romania
2 “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania
Abstract: The left ventricular to right atrial communication, also known as the Gerbode defect, is a very uncommon cardiac anomaly, rarely reported in literature. We present the case of a 63-year-old woman who was admitted to our hospital for altered exercise capacity and diagnosed with a type II Gerbode defect. The communication was initially identified by transthoracic echocardiography and further characterized by magnetic resonance imaging. The case is meant to demonstrate the value of contemporary imaging techniques in the noninvasive assessment of the anatomy and hemodynamics of intracardiac shunts.
Keywords: Gerbode defect, echocardiography, cardiac magnetic resonance imaging
Rezumat: Defectul Gerbode sau comunicarea ventricul stâng atriu drept este o anomalie cardiacă rară, puţine cazuri fiind raportate în literatura de specialitate. Prezentăm cazul unei paciente în vârstă de 63 de ani, care a fost evaluată în serviciul nostru pentru alterarea toleranţei la efort şi diagnosticată cu un defect Gerbode de tip II. Comunicarea a fost inţial identificată prin ecocardiografie transtoracică şi caracterizată suplimentar prin rezonanţă magnetică nucleară cardiacă. Acest caz îşi propune să demonstreze valoarea tehnicilor imagistice contemporane în evaluarea neinvazivă a anatomiei şi hemodinamicii şunturilor intracardiace.
Cuvinte cheie: defect Gerbode, ecocardiografie, rezonanţă magnetică cardiacă
CASE REPORT
A 63-year-old Caucasian woman presented to our hospital for a recent alteration in her exercise capacity. She had been diagnosed with a systolic heart murmur in young adulthood, but, at that time, she underwent no further investigations. Physical exam was normal except for an accentuated, splitted second heart sound and a grade 3/6 systolic murmur at the left sternal border. The electrocardiogram showed a minor right bundle branch block. Transthoracic echocardiography raised suspicion of a communication between the LV and the RA (Figures 1, 2). The velocity of the systolic flow reaching the RA was 4 m/sec. The enlargement of the right chambers, a moderate pulmonic insufficiency and a mild tricuspid regurgitation with moderate pulmonary hypertension were also described. The ratio of pulmonary to systemic flow (Qp/Qs) was 2, consistent with a moderate left to right shunt. The cardiac magnetic resonance imaging (MRI) examination confirmed the presence of a 6 mm defect in the atrioventricular septum, involving the septal leaflet of the tricuspid valve, with subsequent LV to RA communication (Figures 3, 4). The right ventricular (RV) ejection fraction was 38%.
Since the intracardiac shunt was well tolerated for a long period of time and the patient was only mildly symptomatic, we decided for a conservative approach with regular follow-ups.
The Gerbode defect is a very rare cardiac anomaly that exists in congenital1 and acquired forms (secondary to trauma2, infective endocarditis3, myocardial infarction4 or valve surgery5).
The definition of a Gerbode defect, according to the Society of Thoracic Surgeons is a true, direct, left ventricular to right atrial communication, located in the membranous septum6. The most common, indirect type of communication, is from the LV, through a ventricular septal defect into the RV and then, through a defect in the septal leaflet of the tricuspid valve, into the RA1.
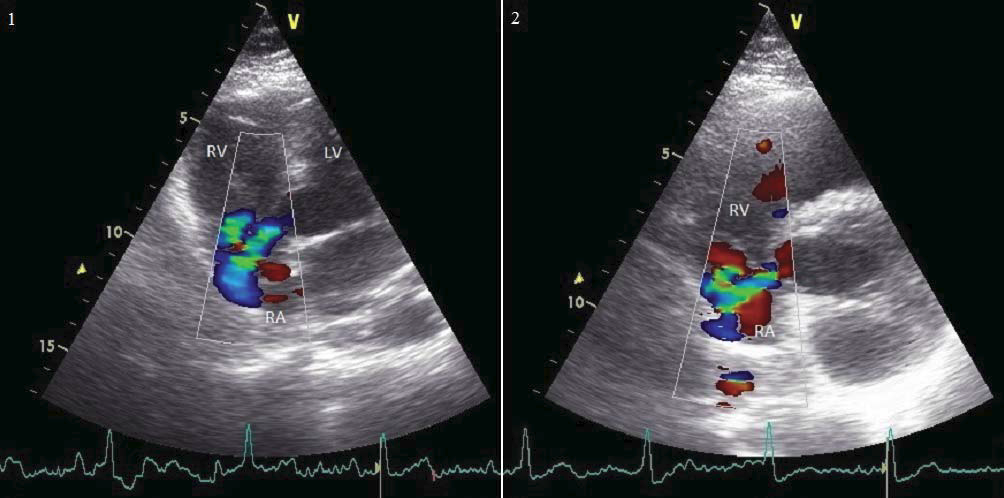
Figure 1,2. Colour Doppler transthoracic echocardiographic images (1 – apical 5 chamber view; 2 – parasternal short axis view): systolic flow between
the LV and RA.
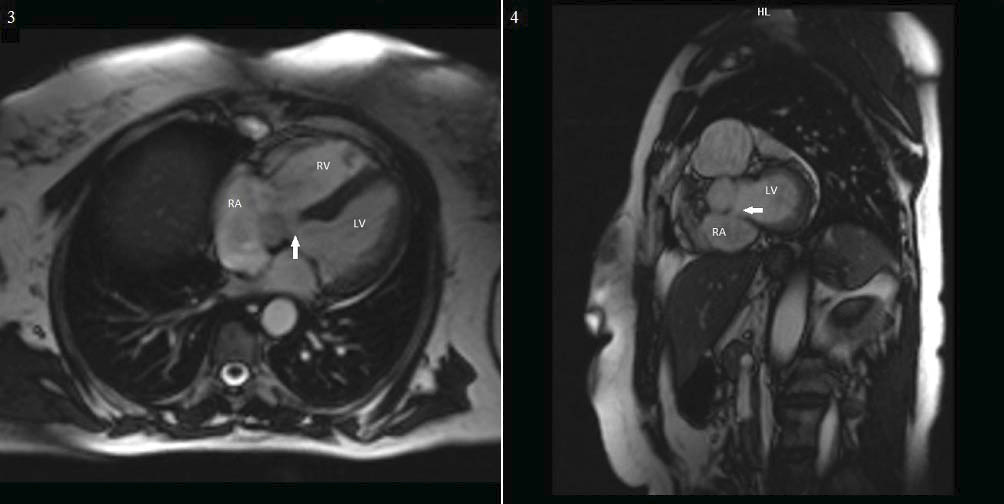
Figure 3,4. Cardiac MRI (3 – transversal and 4 – sagittal) views confirming the Gerbode defect (arrows).
This case demonstrates the value of contemporary imaging techniques such as echocardiography and cardiac magnetic resonance imaging in noninvasively assessing the anatomy and hemodynamics of intracardiac shunts. The data they provide influence clinical decision making and guide the therapeutic surgical or interventional procedures.
Acknowledgements: We would like to thank Dr. Irinel Oancea, from “Phoenix” Diagnostic Clinic, ClujNapoca, for her interpretation of the cardiac MRI examination.
Conflict of interests: none declared.
References
1. Gerbode F, Hultgren H, Melrose D, Osborn J. Syndrome of left ventricular-right atrial shunt; successful surgical repair of defect in five cases , with observation of bradycardia on closure. Ann Surg 1958;148:433-46.
2. Sasaki N, Shimoyama M. Aquired supravalvular type of left ventricular to right atrial communication following non-penetrating cardiac trauma caused by traffic accident. Heart 2003;89:341.
3. Velebit V, Schöneberger A, Ciaroni S, Bloch A, Maurice J, Christenson JT et al. ‘Acquired’ left ventricular to right atrial shunt (Gerbode defect) after bacterial endocarditis. Tex Heart Inst J 1995;22:100-2.
4. Doig JC, Au J, Dark JH, Furniss SS. Post-infarction communication between a left ventricular aneurism and the right atrium. Eur Heart J 1992;13:1006-7.
5. Dadkhah R, Friart A, Leclerc JL, Moreels M, Haberman D, Lienart F. Uncommon acquired Gerbode defect (left ventricular to right atrial communication) following a tricuspid annuloplasty without concomitant mitral surgery. Eur J Echocardiogr 2009;10(4):579-81.
6. Jacobs JP, Burke RP, Quintessenza JA, Mavroudis C. Congenital Heart Surgery Nomenclature and Database Project: ventricular septal defect. Ann Thorac Surg 2000;69(Suppl):S25-35.
 This work is licensed under a
This work is licensed under a