Marin Postu1,2, Nicolae Carstea1,3, Sanda Postu-Plugaru2, Lucian M. Predescu1,3
1 “Prof. Dr. C. C. Iliescu” Emergency Institute for Cadiovascular Diseases, Bucharest, Romania
2 “Ares” Centers of Excellence in Interventional Cardiology and Radiology, Bucharest, Romania
3 „Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
Abstract: Despite the recent developments that have been made in the field of percutaneous left main intervention, the treatment of distal LM bifurcation remains challenging. Elective two-stent techniques, none of which has been proven superior to the others, are frequently used in patients with severely diseased distal left main and true Medina 1,1,1 bifurcation lesion. From those two-stent techniques, with the Culotte technique we can achieve an optimal reconstruction of distal left main bifurcation. The culotte technique can be technically demanding when used with balloon expandable stents. But, the new self-expandable stents with a balloon delivery system can overcome many limitation of classical balloon expandable stents and it can facilitate the Culotte technique in distal left main stenosis. We present the case of a 74-year-old male patient with Medina 1,1,1 distal left main stenosis treated by Culotte technique with the new Stentys Xposition S stent (a self expandable drug eluting stent with balloon delivery system).
Keywords: left main stenosis, culotte technique, percutaneous coronary intervention, self expandable stent
Abstract: În ciuda recentelor progrese care au fost făcute în domeniul angioplastiei de trunchi comun arteră coronară stângă percutanată, tratamentul leziunilor de bifurcaţie trunchi comun distal rămâne o provocare. Tehnicile cu două stenturi, deşi nici una dintre ele nu s-a dovedit a fi superioară celeilalte, sunt frecvent utilizate la pacienţii cu leziuni Medina 1,1,1 de trunchi comun distal arteră coronară stângă. Din aceste tehnici cu două stenturi, cu tehnica Culotte putem realiza o reconstrucţie optimă a bifurcaţiei trunchiului comun. Tehnica culotte poate fi dificilă din punct de vedere tehnic, mai ales atunci când sunt utilizate stenturi balon expandabile. Dar, noile stenturi auto expandabile cu un sistem de livrare pe balon pot depăsi multe limitări ale stenturilor pe balon şi pot facilita tehnica Culotte în stenoza de trunchi comun arteră coronară stângă. Prezentăm cazul unui pacient în vârstă de 74 de ani, de sex masculin, cu leziune Medina 1,1,1 trunchi comun distal tratată prin tehnica Culotte cu noul stent Stentys Xposition S (un stent farmacologic activ autoexpandabil cu sistem de livrare pe balon).
Cuvinte cheie: Stenoza trunchi comun, tehnica Culotte, interventie coronariana percutana, stent autoexpandabil
INTRODUCTION
The optimal stenting strategy for the treatment of unprotected left main coronary bifurcation lesions remains uncertain. To choose the best left main stenting technique we must take into account many lesion characteristics. Besides the technique used, the final result is highly influenced by the type of stent choice.
CASE REPORT
We present the case of a 74-year-old male patient was admitted for aggravated chest pain. He had long-standing hypertension, dyslipidemia, class 2 obesity and moderate renal impairment (glomerular filtration rate = 54 ml/min). Clinical examination revealed a grade 2/6 systolic murmur at the apex, abdominal obesity and the rest of clinical exam was unremarkable. Resting electrocardiogram showed sinus rhythm, heart rate = 68 bpmin, ST depression of 1 mm in the precordial leads and ST elevation of 1 mm in aVR. Transthoracic echocardiography revealed a preserved left ventricular ejection fraction of 55% without wall motion abnormalities and a mild mitral regurgitation. The patient was treated with dual antiplatelet therapy (100 mg per day of aspirin and 90 mg twice a day of ticagrelor), beta-blocker, calcium-channel blocker, angiotensin converting enzyme inhibitor and high dose statin.
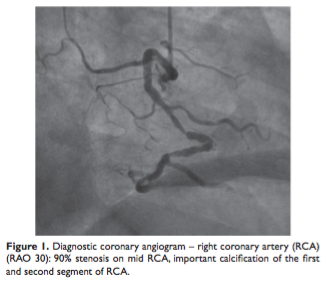
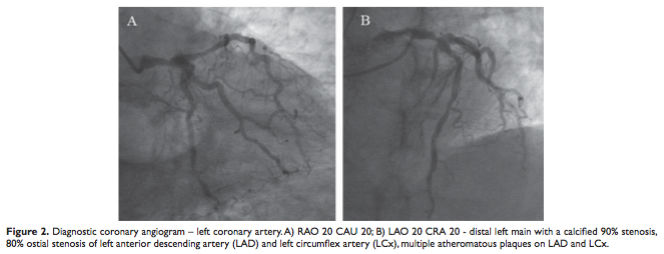
Coronary angiogram was performed using right radial access showing a 90% stenosis on mid right coronary artery (RCA), important calcification of the first and second segment of RCA (Figure 1), distal left main with a calcified 90% stenosis, 80% ostial stenosis of left anterior descending artery (LAD) and left circumflex artery (LCx), multiple atheromatous plaques on LAD and LCx (Figure 2). The Syntax Score was 27 and the EuroSCORE II was 2.67%.
 Because this patient with multivessel disease had a Syntax score of 27 and a low surgical risk, the first choice of revascularization would have been coronary artery bypass surgery. Because the patient refused surgery, the heart team decided to treat the RCA and left main stenosis by percutaneous coronary intervention (PCI).
Because this patient with multivessel disease had a Syntax score of 27 and a low surgical risk, the first choice of revascularization would have been coronary artery bypass surgery. Because the patient refused surgery, the heart team decided to treat the RCA and left main stenosis by percutaneous coronary intervention (PCI).
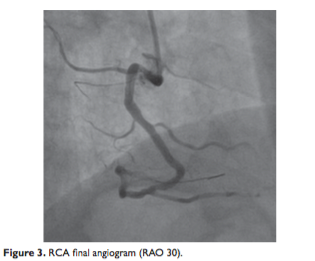
PCI was performed using a 7F right femoral access. We used to engage the RCA ostium an 0.75 Amplatz left guiding catheter, because it offered more support than the right Judkins guiding catheter. Two 0.014” BMW Universal II guidewires were advanced distal in the RCA to enhance the support of the guiding catheter and to act like a buddy wire and to ease the predilatation. The RCA lesion was predilated with a 2.0×20 mm balloon expanded at 12 atmospheres (atm). A 3.5×23 mm Xience Pro stent was deployed at 12 atm and postdilated with a 3.5×15 mm noncompliant balloon inflated at 22 atm. After stent implantation, there was a small dissection distal to the stent, which was covered with a 3.0×12 mm Xience Pro stent expanded at 14 atm, with a good angiographic final result (Figure 3).
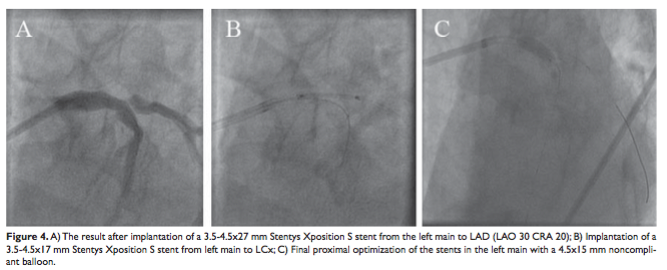
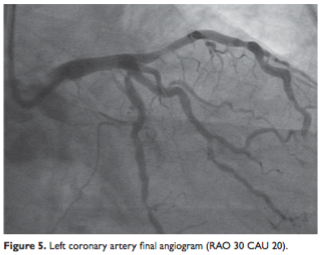
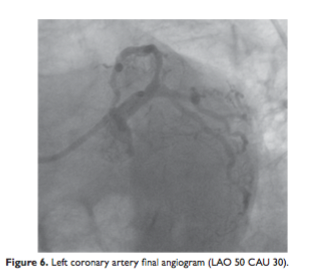
For the left main lesion we used a 7F 4.0 XtraBackup guiding catheter. Two 0,014” BMW Universal II guidewires were placed distal into the LAD and LCx. The left main was predilated toward LAD and LCx using a 3.5×15 mm semicompliant balloon inflated at 12 atm. A 3.5-4.5×27 mm Stentys Xposition S stent was implanted from the left main to the LAD inflated at 8 atm. The stent was postdilated at the bifurcatioen level with a 4.0×15 mm noncompliant balloon inflated at 16 atm (Figure 4A). After rewiring, the stent struts towards LCx were dilated using a 3.0×12 mm semicompliant balloon to facilitate the passage of the second stent. Accordingly to the Culotte technique a second 3.54.5×17 mm Stentys Xposition S was deployed at 8 atm from the left main to the LCx (Figure 4B). The second stent was postdilated with a 4.0×15 mm noncompliant balloon inflated at 16 atm. After rewiring the second stent struts were dilated with a 3.5×15 mm noncompliant balloon from the left main to the LAD. A final postdilatation of the stents in the left main was done with a 4.5×15 mm noncompliant balloon inflated at 16 atm (Figure 4C), with a good final angiographic result (Figure 5 and Figure 6).
Clinical evolution of the patient was good, he was free from angina and he was discharged the following day.
DISCUSSIONS AND IMPLICATIONS FOR CLINICAL PRACTICE
When we are dealing with a distal left main bifurcation lesion, we must take into account many characteristics in order to choose the best bifurcation stenting technique: Medina classification, the difference in diameter between left main, LAD and LCx, the amount of calcium, the angle between LAD and LCX 1. True distal bifurcation lesions may be treated by either a single-stent or by a two-stent strategy. The provisional T stenting and small protrusion, culotte techniques]. More complex lesions may require double-stent strategy (T stenting, TAP, crush, mini crush, culotte, V stenting).
Culotte stenting in left main is a strategy suitable for lesions where the ostium of the LCx is diseased, the angulation between the vessels is <600 (higher risk of plaque shift), and the two vessels are of similar diameter3. The main vessel, usually the left main to the LAD, is stented. A second stent is then passed through the struts of the first stent into the side vessel, leaving an overlap of both stents in the left main. The left main LCx stent is deployed. The procedure is completed with a ‘kissing balloon’ inflation. This technique provides an optimal reconstruction of distal left main bifurcation but with a significant area of stent overlap.
The culotte technique is more technically demanding compared to other bifurcation strategies. But, the use of new generation of stents, like self-expandable stents with open cells facilitates this technique.
Culotte technique in left main is not routinely applied in left main given the relative large size of the left main compared to the available drug eluting stents diameters. Again this problem is solved by self-expandable stents that can reach a diameter in left main with 2 mm higher than the diameter of the LAD or LCX, facilitating a correct vessel wall apposition4.
Another problem with culotte technique was that of the high amount of stent material (the overlap of two stents) left in place in the left main, which determined that this technique to be increasingly less used for a long time5. However, recent studies showed that the clinical outcomes were similar for patients with coronary bifurcation lesions treated with the culotte technique versus other bifurcation stenting techniques, like crush stent technique6.
In this case, we dealt with a Medina 1,1,1 bifurcation lesions of distal left main, with poststenotic dilatation of the origin of LAD and LCX, with important calcifications and with an angle between LAD and LCX less than 600. We used for the treatment of left main bifurcation stenosis the Culotte technique because of the angle between LAD and LCX. Taking into account the high amount of calcium and the difference in diameter between left main, LAD and LCX we chose a coronary self-expandable stent, because of its better conformability and it can be easier appose to the vessel wall. Stentys Xposition S is a self-expandable sirolimus eluting stent that ensure a complete and continuous apposition to vessel wall and from the diameter it was implanted it can achieve a 6 mm maximum vessel diameter. Another important characteristic that made Stentys Xposition S suitable for this lesion was that it can be precisely positioned in order not to miss the lesion. Thanks to these characteristics of the stent, Culotte technique becomes friendlier. We no longer need to make “kissing” and proximal optimization.
We didn’t used intravascular ultrasound to check the final result because the new Stentys Xposition S can achieve a good vessel wall apposition and a continuous expansion.
To our knowledge, this is the first report on treatment of distal left main bifurcation lesion by Culotte technique using the new Stentys Xposition S stent.
Acknowledgment: none declared.
Disclosure: The authors declare that there is no conflict of interest.
References
1. Predescu LM., Zarma L, Platon P. et al. Current treatment of left main coronary artery disease. Cor et Vasa 2015;Article in Press, DOI: http://dx.doi.org/10.1016/j.crvasa.2015.05.007.
2. Fajadet JC, A. Current management of left main coronary artery disease. European heart journal 2012;33:36-50b.
3. Ahn JM, Lee PH, Park SJ. Practical based approach to left main bifurcation stenting. BMC cardiovascular disorders 2016;16:49.
4. Smolka G, Wanha W, Roleder T, Pluta A, Ochala A. Treatment of left main coronary artery stenosis with the STENTYS self-expandable drug-eluting stent a pilot registry. Postepy w kardiologii interwencyjnej = Advances in interventional cardiology 2014;10:226-30.
5. Chen SL, Xu B, Han YL, et al. Clinical Outcome After DK Crush Versus Culotte Stenting of Distal Left Main Bifurcation Lesions: The 3-Year Follow-Up Results of the DKCRUSH-III Study. JACC Cardiovascular interventions 2015;8:1335-42.
6. Kervinen K, Niemela M, Romppanen H, et al. Clinical outcome after crush versus culotte stenting of coronary artery bifurcation lesions: the Nordic Stent Technique Study 36-month follow-up results. JACC Cardiovascular interventions 2013;6:1160-5.
 This work is licensed under a
This work is licensed under a