Monica Roşca1,2, Diana Maftei2, R. Iacob3, C. Călin1,2, Carmen Ginghină1,2, B. A. Popescu1,2
1 “Carol Davila” University of Medicine and Pharmacy Bucharest – Euroecolab Laboratory
2 ”Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases Bucharest
3 Fundeni Clinical Institute, Gastroenterology, Bucharest
Monica Roşca, MD, “Carol Davila” University of Medicine and Pharmacy Bucharest – Euroecolab Laboratory. ”Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases Bucharest
A 25 year old female patient, without a significant medical history is admitted for fatigability and pain in the right hypochondrium for the past 3 months. The abdominal ultrasound reveals two cystic masses in the IInd and IVth hepatic segments and serum tests are positive for Echinococcus Granulosus, confirming the diagnosis of hepatic hydatidosis. A cardiologic exam is considered required in order to complete the protocol.
The echocardiographic examination shows normal dimensions of the left ventricle (LV), a preserved global and segmental LV function. At the level of the medium and apical segments of the inferolateral LV wall, a well-contoured, inhomogenous, cystic mass can be observed, without color flow, containing well defined hypoechogenic areas – suggestive for hydatid cyst. From a short axis parasternal view the mass measures 27/53 mm (Figure 1) and 29/45 mm from the apical long axis view (Figure 2). The echocardiography cannot establish whether the cyst is intramyocardial or intrapericardial. It appears to be in close contact with the inferolateral wall of the LV, without altering intracardiac flow. The color Doppler examination does not reveal any hemodinamically significant valvular lesions and the 2D examination does not reveal any pericardial effusion. The diagnosis was confirmed by cardiac MRI, locating the mass within the wall of the LV, in the medio-lateral segments (Figure 3). The mass has a maximum diameter of 5.7 mm and the minimum thickness of the restante myocardium toward LV cavity measures 0.5 mm. The imaging diagnosis is LV intramyocardial hydatid cyst. In contrast MRI, no positive late gadolinium enhancement was revealed, demonstrating the absence of LV myocardial fibrosis or scarring.
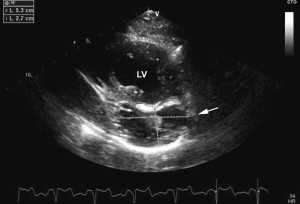
Figure 1. Transthoracic echocardiography, short axis parasternal view at the level of the papillary muscles: at the level of the inferior LV wall a cystic mass (arrow) with a well defined contour and inhomogenous echogenicity is observed. It measures 27/53 mm at this level.
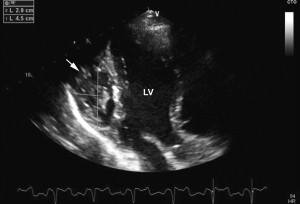
Figure 2. Transthoracic echocardiography, apical long axis view – the mass measures 29/45 mm (arrow), without the possibility of determining its exact location (intramyocardial / pericardial).
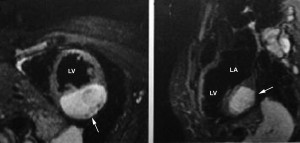
Figure 3. Cardiac MRI – the mass has a maximum diameter of 5.7 mm, is located in the LV myocardium at the level of the medio-lateral segments (arrows). The minimum thickness of the left ventricle’s myocardium, in relation to the ventricular chamber, is 0.5 mm.
Cardiac hydatidosis is a rare pathology, usually affecting the heart as a result of a systemic infection. The most frequent locations of hydatid cysts are the liver (65%) and the lungs (25%). In rare cases hydatidosis affects the heart (0.02-2%), the LV being the most common site (55-60%)(with intramyocardial location and subepicardial extension), followed by the interventricular septum, the right ventricle and rarely the pericardium or atrial myocardium. The echocardiography, computer tomography and cardiac MRI can evaluate the morphology and relations with the adjacent structures. Echocardiography is the standard imaging method used in the diagnosis of cardiac hydatidosis due to its availability, high sensitivity and the potential of determining the hemodynamic consequences. Computer tomography is superior to any other method in revealing parietal cystic calcifications, but the quality of the information regarding the anatomy of the cyst’s internal structures is better with MRI, this being the preferred technique for the post therapy follow-up. The standard treatment for heart hydatidosis is surgery. Antiparasitic treatment (albendazole) is reserved for elderly patients, without hemodynamic impairment, or perioperative, in order to prevent recurrences or intraoperatory dissemination.
Conflict of interests: The authors declare no conflict of interest.
 This work is licensed under a
This work is licensed under a