Lucia Egher1, D. Gherasim1, C. Cosmin1,2, Carmen Ginghină1,2
Article received on the 27th of September 2012. Article accepted on the 8th of November 2012.
1 ”Prof. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases Bucharest
2 “Carol Davila” University of Medicine and Pharmacy Bucharest
Dr. Lucia Egher, ”Prof. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases Bucharest
The stress test remains the most frequently used method for diagnosing patients suspected of suffering from cardiac ischemia. Compared to ST depression, a positive criterion when it exceeds 0.1 mV measured at 80 ms from J point, ST elevation (in the absence of necrosis q waves) is a much rarer phenomenon (its estimated incidence is between 0.5% and 6.5%). It represents severe transmural ischemia, occurring after a spasm or as a result of the occlusion of a coronary artery.
Unlike ST depression, its elevation can reveal the location of the ischemia. In the context of an acute coronary syndrome, ST elevation in the aVR lead is associated with a tight left main stenosis or with the proximal occlusion of the anterior descending artery1,2.
56 year old patient, smoker, dyslipidemic, obese, without a personal history of heart disease, accuses chest pain, atypical for angina, with a recent debut, initially interpreted in the context of a thoracic trauma as a result of falling. The probability for the existence of an ischemic cardiac disease prior to the test is estimated as intermediary, taking into consideration the age, sex and race.
The treadmill stress test employing the Bruce protocol was interrupted after 4 minutes and 40 seconds at the maximum heart rate of 136 bpm (83% of the theoretical maximum heart rate corresponding to the age), functional capacity of 7.0 METS, due to the occurrence of angina pectoris and significant terminal phase modifications. The test is intensely positive given the amplitude and persistence of the ST modifications, as well as the number of leads in which they appeared. Studies associate this aspect with the presence of severe multivascular disease and left main stenosis.
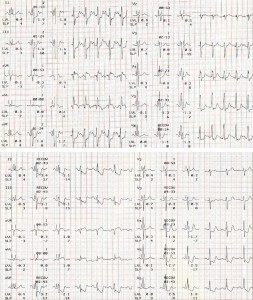
Figure 1. ECG performed during the stress test. A. During the effort, second Bruce stage, horizontal depression of the ST segment in the DII, DIII, aVF, V4-V6 leads and ST elevation in the aVL and aVR leads. B. After the effort, in the recovery period, the terminal phase modifications still persist.
The coronarography revealed a 90% stenosis of the left main, the occlusion of the circumflex artery and that of an intermediary branch, without lesions on the right coronary artery.
The particularity of the case is the severity of the coronary disease exposed by the test and confirmed angiographically, for a patient presenting few symptoms and nonspecific clinical manifestations. Emergency surgical revascularization was performed: aorto-coronary bypass for left main stenosis using internal mammary artery and internal saphenous vein for the intermediary branch. Postoperative evolution was favorable.
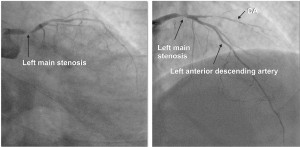
Figure 2A, B. The coronarography shows a 90% left main stenosis and the occlusion of the circumflex artery (CA).
Discussions
- ST elevation in the aVR lead induced by the stress test can be interpreted as a marker for a significant left main or proximal anterior descending artery stenosis (75-80% sensitivity, 94% negative predictive value and positive predictive value of 44%)3.
- ST elevation in aVL induced by the effort (in patients without a personal history of anterior myocardial infarction) can be correlated with ST depression in the leads corresponding to the inferior area and with the amplitude of the R wave in aVL. In more than 90% of the cases ST elevation appears when the amplitude of the R wave in aVL is lesser than 0.5 mV. ST elevation present in the aVL lead has a 16% sensitivity, 90% specificity and a positive predictive value of 57% as a predictive factor4.
- The stress effort is safe for patients with left main lesions, although the documented left main stenosis represents a relative contraindication for performing the stress test.
Conflict of interests: none declared.
Bibliography
1. E. Apetrei, I. Stoian Electrocardiografie-110 exemple, Ed. Info Medica, 2002; 65-248.
2. H. Wellens, M.Conover The ECG in Emergency Decision Making, 2nd Ed Elsevier Saunders 2006; 1-54.
3. S. Uthamalingam, H. Zheng, M. Leavitt, E. Pomerantsev et al Exercise-Induced ST-Segment Elevation in ECG Lead aVR Is a Useful Indicator of Significant Left Main or Ostial LAD Coronary Artery Stenosis, J Am Coll Cardiol Img 2011; 4:176-86.
4. T. Chikamori, T. Hamada, H. Seo et al Determinants of Exercise-Induced ST-Segment Displacement in the aVL Lead in Patients With Known or Suspected Coronary Artery Disease, Jpn Circ J 1999; 63: 104-110.
 This work is licensed under a
This work is licensed under a