A. Negoiţă, M. Postu, D. Deleanu
Article received on the 23rd May 2012. Article accepted on the 28th May 2012.
1 „Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases, 258, Fundeni Street, Bucharest
„Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases, 258, Fundeni Street, Bucharest
Male, 59 years old, known with arterial hypertension, dyslipidemia, smoker presented at the emergency room 3 hours after the beginning of a retrosternal pain, typical for angina. The patient is brought after a resuscitated cardiopulmonary arrest, being intubated in the emergency room, mechanically ventilated, with a BP of 80/60 mmHg. Initial ECG shows a sinus rhythm with AV of 90 bpm, a maximum 1mm ST segment elevation in DIII, aVR, right leads with negative T waves at this level, ST segment depression in aVL (Figure 1). Based on the clinical and paraclinical data, the diagnosis of acute coronary syndrome with ST segment elevation is set 3 hours from the resuscitated cardiopulmonary arrest. Emergency coronary surgery is decided.

Figure 1. ECG: Sinus rhythm, 90 bpm, ST segment elevation in DIII, aVR, right leads of maximum 1mm with negative T waves at this level, ST segment depression in aVL.
When injecting the left arterial coronary, important diffuse spasm isnoted at the level of the left main coronary artery, the anterior dedcending artery and the circumflex artery with distal occlusion on the circumflex artery (Figure 2A). Nitroglycerine is administrated intracoronary and the remission of spasm at the level of the the whole left coronary artery is noted (Figure 2B).
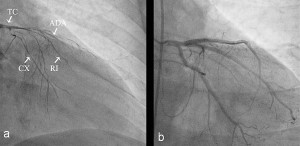
Figure 2. Coronary angiography – injection in the left coronary artery- one can notice the left main (TC), the anterior descending artery (ADA) and the circumflex artery (CX) with important diffuse spasm producing occlusion of the 2nd segment of the anterior descendent aorta and distal oclusion at the level of the CX (Figure 2A). After intracoronary nitroglycerine administration we noted the absence of the spasm at the level of the whole left coronary artery (Figure 2B).
When injecting the right coronary artery, we noted the oclusion of the proximal segment with intraluminal thrombotic aspect (Figure 3). Taking into consideration the spasm existent at the level of the left coronary artery, nitroglycerin is repeateadly administred intracoronary leading to a complete remission of the spasm for the whole blood vessel (Figure 3B).
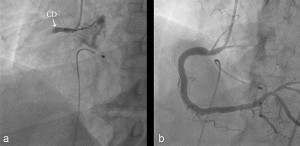
Figure 3. Coronary angiography – injection in the right coronary artery (CD) – proximal oclusion, with intraluminal thrombotic aspect (Figure 3A). Figure 3B – complete complete remission of the spasm after intracororonary nitroglycerine administration.
Bibliography
1. Rashid H, Marshall RJ, Diver DJ, Breall JA. Spontaneous and diffuse coronary artery spasm unresponsive to conventional intracoronary pharmacological therapy: a case report. Catheter Cardiovasc Interv 2000; 49:188–91.
2. Yasue H, Nakagawa H, Itoh T, Harada E, Mizuno Y. Coronary artery spasm – clinical features, diagnosis, pathogenesis, and treatment. J Cardiol 2008; 51:2–17.
 This work is licensed under a
This work is licensed under a