Lucian Predescu1,2, Marin Postu1, Lucian Zarma1, Marian Croitoru1, Pavel Platon1,2, Adrian Bucșa1, Adrian Mereuță1,2, Dan Deleanu1
1 Emergency Institute for Cadiovascular Diseases “Prof. Dr. C. C. Iliescu”, Bucharest
2 University of Medicine and Pharmacy „Carol Davila”, Bucharest
All the abnormalities in term of number, origin, course and termination of coronary arteries, which are unusual in the general population enters in the group of congenital coronary artery anomalies. The incidence of coronary anomalies varies widely between 1% and 5% 1. Anomalies of origin of the coronary arteries are not always benign and some of them caries a risk of inducible myocardial ischemia and sudden cardiac death (SCD). The sensitivity of electrocardiographic and echo cardiographic stress testing in detecting inducible myocardial ischemia can be very low in patients with coronary artery anomalies. An intramural course, an acute angle of takeoff, slit like ostium or a course between aorta and the pulmonary trunk are associated with a great risk of myocardial ischemia. Anomalous pulmonary origin of the coronary arteries has the greatest risk for myocardial ischemia and SCD; most infants dies within one year (95%). The most common variant of this syndrome is an anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA), but any coronary artery (left anterior descending artery – LAD, circumflex – LCx or right coronary artery – RCA) may originate from the pulmonary artery (Figure 1)2. The anomalous coronary artery origin from the opposite sinus bears a risk of myocardial ischemia and SCD if the course of the artery is between aorta and pulmonary trunk. Two third of patients with aberrant left main coronary artery arising in the right coronary sinus of Valsalva dies suddenly, 75% during exercise (Figure 2) 3. Anomalous LCx from the RCA or right sinus is the most frequent anomaly of origin of the coronary arteries and it is mostly a benign finding (Figure 3). More rarely the LAD can originate from the RCA. One third of patients with anomalous RCA from the left sinus dies suddenly, mainly because of the compression of RCA between aorta and the pulmonary trunk (Figure 4, 5)4. Coronary artery fistulas are a communication between a coronary artery and a cardiac chamber or a major vessel. Patient with coronary artery fistula are mostly asymptomatic but they can develop dyspnea on exertion, pulmonary hypertension if the fistula generate a big shunt (Figure 6)5. Conflict of interests: none declared.
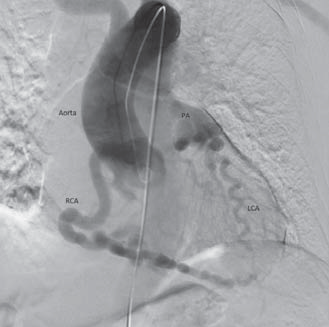
Figure 1.Aortography – right coronary artery (RCA) with origin from the right sinus of Valsalva fills throw collaterals the left coronary artery (LCA) which have an anomalous origin in the pulmonary artery trunk (PA).
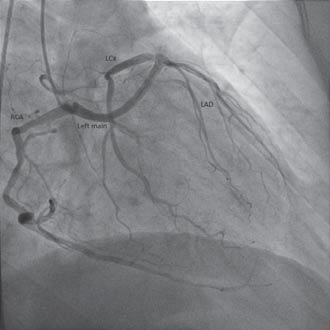
Figure 2. Aberrant left coronary artery with a very long left main arising in the right coronary sinus of Valsalva very close to the origin of right coronary artery (RCA – right coronary artery, LCx – circumflex artery, LAD – left anterior descending artery).
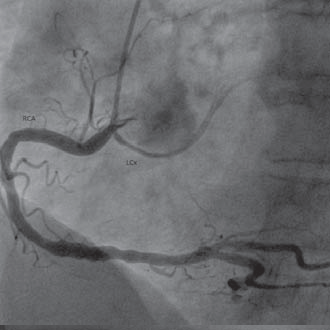
Figure 3. Aberrant circumfl ex artery from the right coronary artery in the right coronary sinus of Valsalva (RCA – right coronary artery, LCx – circumflex artery).
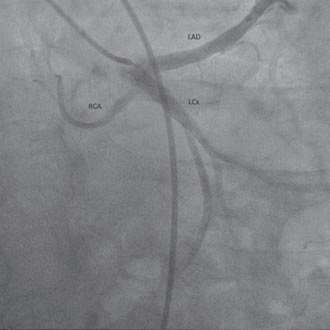
Figure 4. Anomalous right coronary artery from the left coronary artery (RCA – right coronary artery, LCx – circumflex artery, LAD – left anterior descending artery).
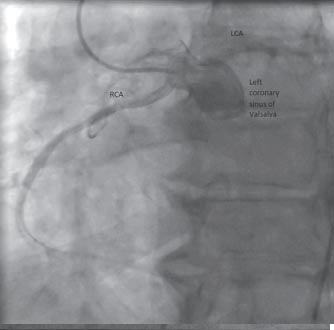
Figure 5. Anomalous right coronary artery from the left coronary sinus of Valsalva (RCA – right coronary artery, LCA – left coronary artery).
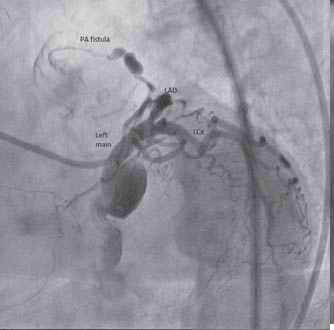
Figure 6. Coronary artery fistula between left coronary artery and pulmonary artery (LCx – circumflex artery, LAD – left anterior descending artery, PA – pulmonary artery).
 This work is licensed under a
This work is licensed under a