A. Negoiță, F. Purcarea, M. Croitoru, D. Deleanu
Article received on the 12th of February 2013. Article accepted on the 28th of February 2013.
“Prof. Dr. C. C. Iliescu” Emergency Institute of Cardiovascular Diseases, Bucharest, Romania
Negoita Adrian, MD, “Prof. Dr. C. C. Iliescu” Emergency Institute of Cardiovascular Diseases, 258 Fundeni Street, District no. 2, 022328, Bucharest, Romania.
We present the case of an 85 year old woman with a personal history of hypertension and dyslipidemia, brought by the ambulance to the emergency room two hours after the debut of an intense retrosternal chest pain. During transportation to the emergency room the patient suffered an episode of conscience loss. The EKG performed in the ambulance revealed a ventricular tachycardia episode, electro-converted to sinus rhythm.
The clinical examination performed upon presentation marks a deteriorated state, blood pressure (BP) 70/40 mmHG, heart rate (HR) 35 bpm, EKG shows a IIIrd degree atrioventricular block, ST elevation in DII, DIII, aVF, V4 – V6, (a maximum of 5 mm), ST depression in DI, aVL , V1-V3. The echocardiography reveals a moderate systolic dysfunction (ejection fraction (EF) 40%) and segmentary kinetic abnormalities of the lateral and inferior walls, with severe mitral regurgitation.
The patient is immediately brought to the catheterization laboratory, where an emergency angiography is performed, after the implantation of a temporary stimulation electrode. The coronarography discovers an acute thrombotic occlusion both in the second segment of the circumflex artery, as well as in the first segment of the right coronary artery (RCA) with TIMI 0 distal flux in both vessels. Thromboaspiration with the extraction of thrombotic material is performed on both occlusions and tight stenosis areas can be observed on both coronary vessels, requiring stent implantation.
Postoperatory, the patient‘s evolution was favorable, she was hemodynamically stable, with a significant improvement concerning the degree of mitral regurgitation (IInd degree) and the remission of the atrioventricular block.
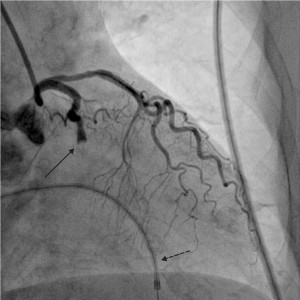
Figure 1. Acute thrombotic lesion on the IInd segment of the circumflex coronary artery (CxA), TIMI 0 flux (continuous arrow), cardiostimulation electrode placed in the right ventricle (RV) (dotted arrow).
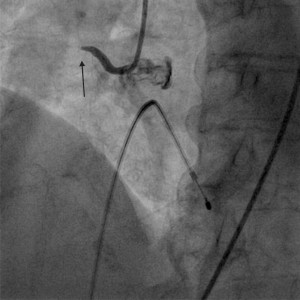
Figure 2. Acute right coronary artery thrombotic lesion in the Ist segment. Timi 0 flux (continuous arrow).
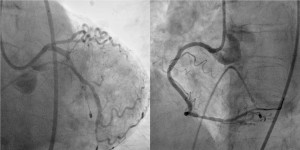
Figure 3. Final result after thromboaspiration and stent implantation on the CxA and RCA, with TIMI III distal flux.
 This work is licensed under a
This work is licensed under a