Lucian Predescu1, Marin Postu1, Pavel Platon1, Mihaela Rugina1, Madalina Gavanescu1, Marian Croitoru1, Adrian Bucsa1, Lucian Zarma1, Dan Deleanu1
1 Emergency Institute for Cadiovascular Diseases “Prof. Dr. C. C. Iliescu”,Bucharest, Romania
Contact address:
Lucian Predescu, MD
Emergency Institute for Cadiovascular Diseases “Prof. Dr. C. C. Iliescu”, sos. Fundeni 258, sector 2, 022328, Bucharest, Romania.
We present a case of a 65 years old male patient, admitted with intermittent claudication of lower limbs at 200 meters. The cardiovascular risk factors of the patient were: stage III hypertension, dyslipidemia and smoking. The results of a clinical examination were unremarkable. A lower limbs arterial Doppler echography was made, that showed 50-60% stenosis with calcified plaques in both superficial femoral arteries and we proceeded to peripheral arteriography.
During the procedure, after sheath has been introduced, a local hematoma rapidly developed, which was treated by manual compression. Terminal aorta, common and external iliac arteries, and common femoral arteries had plaques and calcifications without significant stenosis. The angiogram showed right superficial femoral artery blood extravasation at the level of vascular access, an abnormal image that raise the suspicion of an extensive dissection (Figure 1), acute thrombotic occlusion of right popliteal artery and permeable left popliteal artery with calcified plaques (Figure 2), absent blood flow below the right knee and normal right calf arteries. Because the suspicion of an extensive dissection persisted, we removed the right femoral sheath and we achieved hemostasis by manual compression. We used a left femoral approach (5F) with cross over and the new images invalidate the diagnosis of superficial femoral artery dissection (Figure 3) and confirm the acute thrombotic occlusion of right popliteal artery (Figure 4).
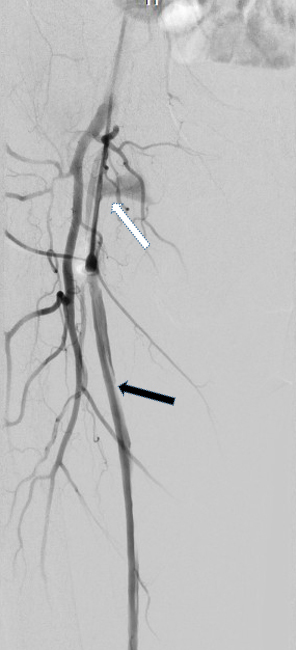
Figure 1. Superficial femoral artery blood extravasation at the level of vascular access (white arrow) and an abnormal image that raise the suspicion of an extensive dissection (black arrow).

Figure 2. Acute thrombotic occlusion of right popliteal artery (arrow). Permeable left popliteal artery with calcified athermanous plaques.

Figure 3. Angiogram of the right femoral artery after cross over from the left femoral artery. There are no signs of dissection.

Figure 4. Acute thrombotic occlusion of right popliteal artery with absent blood flow below the right knee (arrow).
Local Heart Team had to decide between: 1) thrombolysis, which is a safe and effective alternative to surgery with a 86% success rate, but with high risk of hemorrhagic complications1, 2) popliteal thromboaspiration, which has excellent early and mid-term results in selected cases, with short occlusions2 and 3) arterial embolectomy using Fogarty catheter. The choice was for popliteal thromboaspiration. We used a right common femoral artery antegrade approach, with a 7F sheath. Repetitive and progressive direct catheter thromboaspiration using a 7F multipurpose catheter until the level of calf arteries has been done with massive thrombus extraction (Figure 5). The final result was good, with repermeabilization of right popliteal artery and minimal residual thrombus in the anterior tibial artery (Figure 6). Unfractionated heparin was administrated for 24 hours with good clinical evolution. Thrombophilia tests were positive for a protein S deficiency.
Although peripheral arteriography is a relatively safe procedure (major vascular complication rate 1.9%), it remains an invasive investigation that carries a risk of major complications3. It’s important of balancing the risks of the procedure with the firmness of the indications and the benefits of the procedure for every patient. Percutaneous thrombus aspiration in acute thrombotic occlusion of the popliteal artery is an effective and safe alternative to surgery.
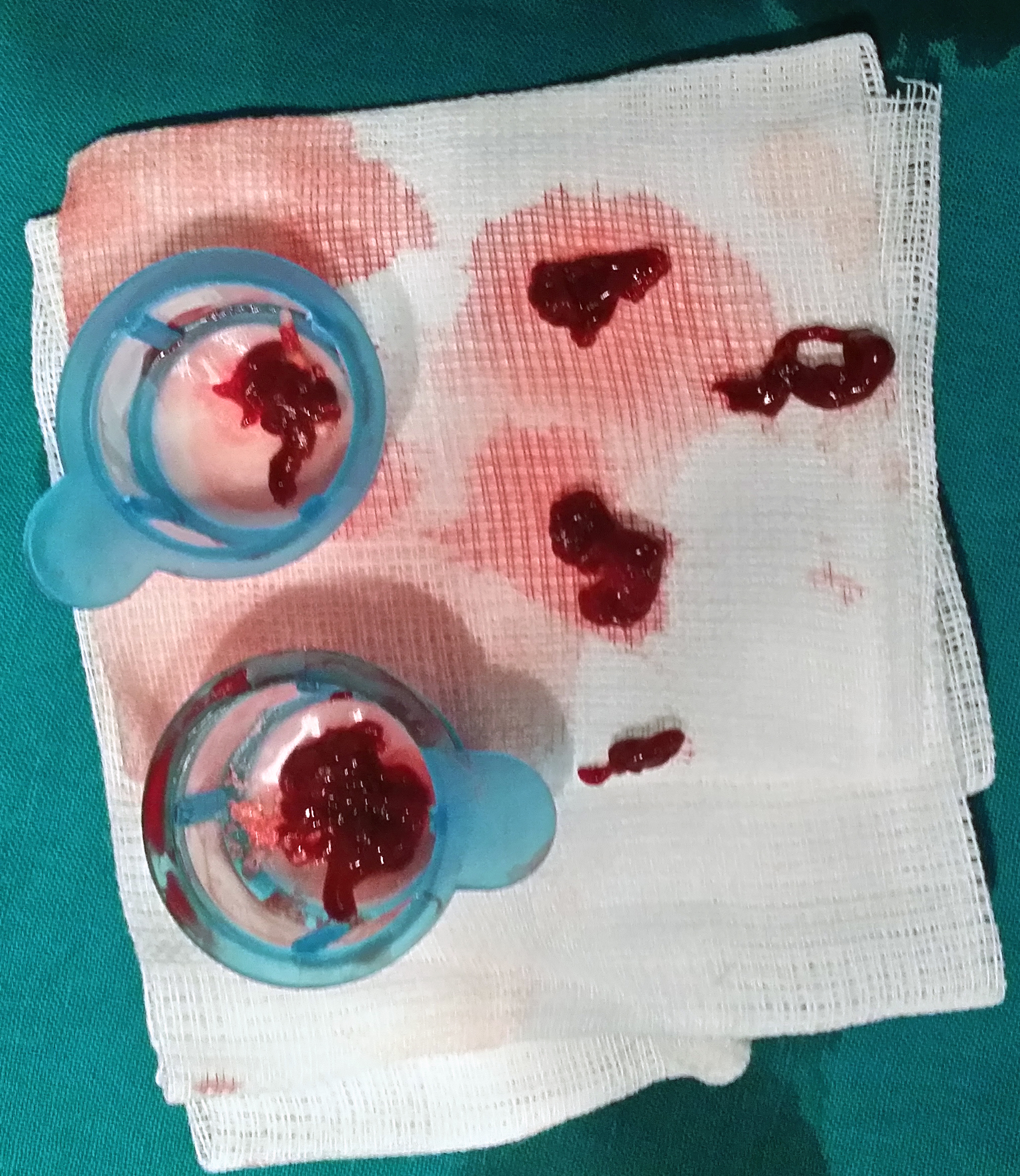
Figure 5. Massive thrombus extraction after popliteal direct catheter thromboaspiration.

Figure 6. Final result – repermeabilization of right popliteal artery with minimal residual thrombus in the anterior tibial artery (arrow).
Conflict of interests: none declared.
References:
1. Van Damme, H., et al., Intra-arterial thrombolysis of thrombosed popliteal artery aneurysm. A series of six cases. Acta Chir Belg, 2006. 106(6): p. 679-83.
2. Desgranges, P., et al., Acute occlusion of popliteal and/or tibial arteries: the value of percutaneous treatment. Eur J Vasc Endovasc Surg, 2000. 20(2): p. 138-45.
3. Egglin, T.K., et al., Complications of peripheral arteriography: a new system to identify patients at increased risk. J Vasc Surg, 1995. 22(6): p. 787-94.
 This work is licensed under a
This work is licensed under a