Marin Postu1, Lucian Predescu1, Peep Laanmets2, Ion Bostan1, Carmen Ginghina1, Mircea I. Coman1
1 “Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases, Bucharest, Romania
2 North-Estonia Medical Centre, Tallinn, Estonia
We present the case of a 65-year-old male patient admitted in our institute for canadian class II angina. His cardiovascular risk factors were dyslipidemia and sta-ge III hypertension. The patient is known with coronary multivessel disease and a coronary artery bypass graft surgery (CABG) with saphenous venous grafts (SVG) on left anterior descending artery (LAD), first marginal artery and right coronary artery (RCA) (one year ago). Coronary angiogram was repeated showing the occlusion of SVG on first marginal branch and RCA, and severe stenosis at the anastomosis site of SVG with LAD which was treated with a drug eluting stent (DES) implantation (6 months ago). The resting electrocardiogram was unremarkable and the transthoracic echocardiography showed a mild left ventricular systolic dysfunction. Coronary angiogram performed by bilateral injection showed a proximal and long occlusion of left circumflex artery (LCx), the occlusion of LAD after the first septal branch, a permeable SVG on distal LAD (Figure 1) and a very long proximal occlusion of RCA (Figure 2). Using bilateral injections (in SVG on LAD and left coronary artery) the left circumflex artery was opened using an ante-grade approach with a GAIA second guidewire and Corsair Pro microcatheter (Figure 3). Using bilateral injection (in left coronary artery and RCA) the RCA was opened using a retrograde approach and the reverse CART (controlled antegrade and retrograde tracking) technique. We used the first septal branch proximal to the LAD occlusion to pass in distal RCA a Corsiar Pro microcatheter using a Sion Blue and Sion Black guidewire. The reverse CART was done using two Gaia second guidewires and a 2.5 mm semicompliant balloon. After externalization of the guidewire we switched to an antegrade approach (Figure 4). Three DES were implanted with a good final angiographic result of RCA (Figure 5).
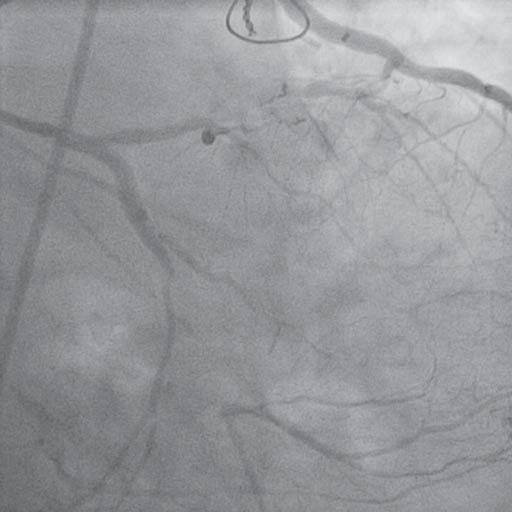
Figure 1. Bilateral injection (in saphenous venous graft (SVG) on left anterior descending artery (LAD) and in left coronary artery) showed a proximal and long occlusion of left circumflex artery, the occlusion of LAD after the first septal branch, a permeable SVG on distal LAD.
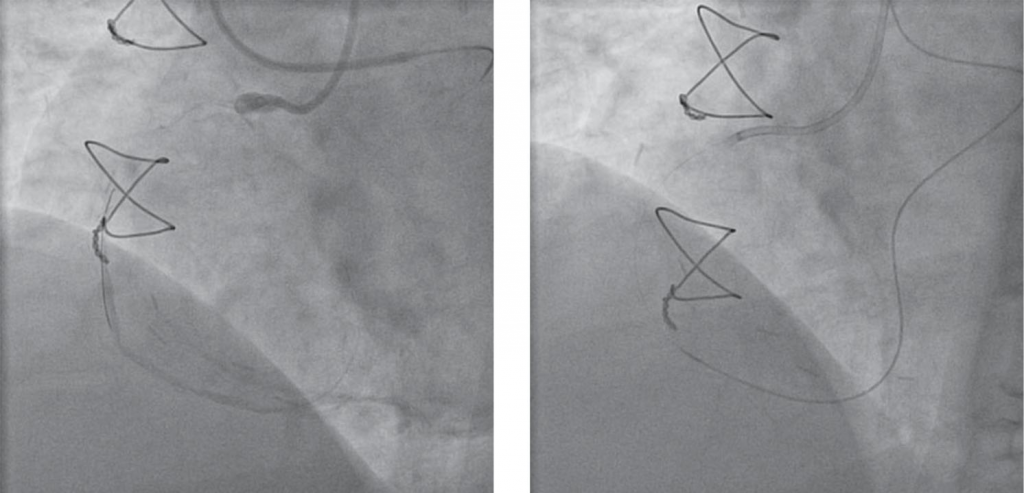
Figure 2. Bilateral injection (in left coronary artery and right coronary artery (RCA)) showed a very long proximal occlusion of RCA.
Figure 4. Externalization of the guidewire during right coronary artery percutaneous coronary intervention.
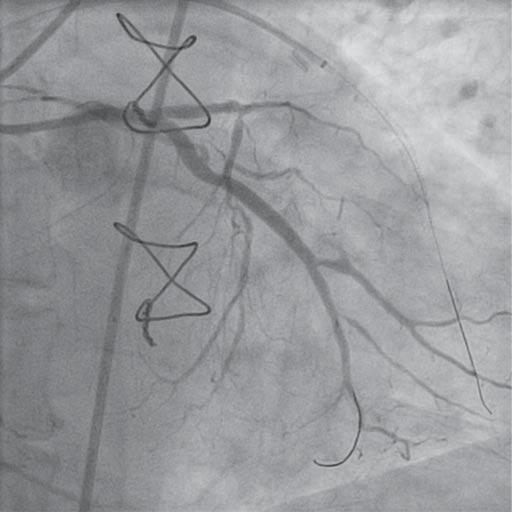
Figure 3. Left coronary artery after opening the left circumflex artery by an antegrade approach.
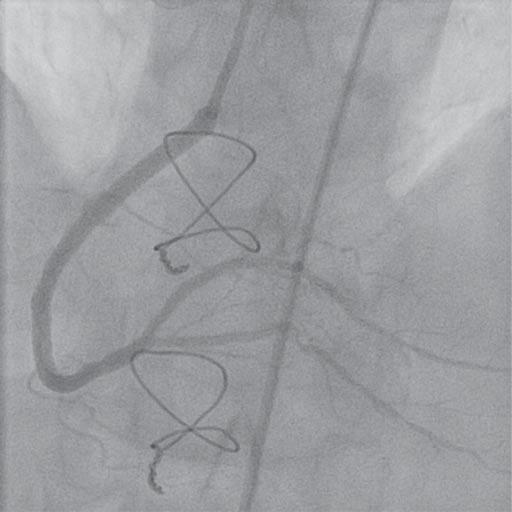
Figure 5. Right coronary artery after percutaneous coronary intervention using a retrograde approach.
 This work is licensed under a
This work is licensed under a