Monica Roşca1,2, Anamaria Avram2, Carmen Ginghină1,2, B. A. Popescu1,2
Article received on the 27th of August 2012. Article accepted on the 31st of August 2012
1 “Carol Davila” University of Medicine and Pharmacy Bucharest – Euroecolab Laboratory
2 “Prof. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases Bucharest
Monica Roşca, “Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases, 258 Fundeni Str., Sector 2, Bucharest, Post Code – 022328. Tel.: 0213180400
A.C., 71 years old, solicits a cardiac evaluation for decubitus dyspnea, orthopnea and voluminous calf edema that started 2 weeks prior to the consultation. The patient reports progressive exertional dyspnea in the preceeding 7 months without any history of heart disease. Three years before present admission he was diagnosed with idiopathic hypereosinophily, for which
he was treated with corticosteroids, with an initially favorable response. Later, the patient did not remain in the attention of the hemathology service, not pursuing any of the periodical check-ups.
The transthoracic echocardiography described normal dimensions of the left ventricle at the basal level, with 2/3 of the apical section occupied by a mass with mixed echogenicity, with partial obliteration of the LV cavity (Figure 1) and a free, circulated lumen extending up to the apex as revealed by the color Doppler flow. The estimated ejection fraction (EF) was 50%, considering the presence of an akinetic apical zone. The volumetric calculation of the EF could not be performed because of the particular distribution of the intracardiac mass (LV potential volumes within normal limits, but severely reduced functional volumes). The pulse wave Doppler analysis of the transmitral diastolic flow (Figure 2) and tissue Doppler of the basal interventricular septum (Figure 3), showed a restrictive diastolic dysfunction of the LV, with high LV filling pressures, due to endomyocardial fibrosis and to the presence of an extensive, non-compliant cardiac wall mass. A minor mitral regurgitation was also revealed. The right ventricle was within normal limits, both functionally and morphologically. The pulmonary systolic arterial blood pressure was estimated at 80 mmHg.
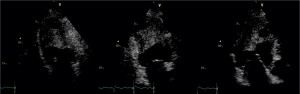
Figure 1. Transthoracic echocardiography, 4, 2 and 3 chamber apical views. The LV has two thirds of the apical section occupied by a mass with mixed echogenicity, apparently without a dissection plane, without mobile elements, with partial obliteration of the LV, with a circulated lumen extending up to the apex.
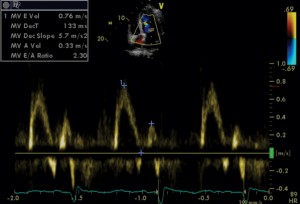
Figure 2. Transthoracic echocardiography, apical 4 chamber view, pulse wave Doppler examination of the transmitral flow: restrictive LV diastolic dysfunction (E/A ratio = 2.3 and EDT = 130 ms).
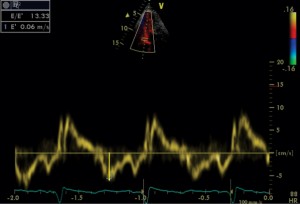
Figure 3. Transthoracic echocardiography, apical 4 chamber view, pulsed wave tissue Doppler imaging of the basal interventricular septum: E’ = 6 cm/sec, E/E’ ratio = 13.
The prevalence of cardiac involvement in hypereosinophilic syndrome exceeds 50%. Loeffler’s endomyocarditis is the classical manifestation, characterized by the fibrous thickening of the endocardium, apical ventricular obliteration and restrictive hemodynamics. The pathogenesis of the cardiac impairment includes 3 stages: acute necrosis, thrombosis and fibrosis. Widely spread, echocardiography was for a long time the most common noninvasive imagistic method used for evaluating the degree of cardiac involvement in hypereosinophilic syndrome, but the gold standard remains endomyocardial biopsy. Recently, cardiac magnetic resonance became the preferred method of investigation, useful for tissue and functional characterization, guided biopsy samples and for revealing the existence of a dissection plane between the intracardiac mass and the endocardium, in the eventuality of a surgical resection.
 This work is licensed under a
This work is licensed under a