Maria Viorela Dobroiu1,2, Ion Relu Ondin Zaharia1,2, Diana Cornelia Nistorescu1,2, Camelia Nicolae1,2, Ioan Tiberiu Nanea1,2
1 „Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
2 Departament of Internal Medicine and Cardiology, „Prof. Dr. Th. Burghele” Clinical Hospital, Bucharest, Romania
Abstract: Background – Ergometer bicycle and treadmill exercise tests are used for diagnosing ischemic heart disea-se. Measurement of blood pressure (BP) during exercise test is mandatory. Gender, weight, body mass index(BMI) infl u-ence BP response during exercise. But how are controlled hypertensive patients reacting to exercise testing? Aim – BP response assessment during exercise test in controlled hypertensive patients in relation to gender, weight, BMI. Method – 58 controlled (normal BP values in ambulatory blood pressure monitoring (ABPM) for minimum 2 weeks) hypertensive patients (54.78±11.41years) underwent treadmill or bicycle submaximal exercise test (target heart rate (220-age-years) x85%). They were assessed with ABPM and transthoracic echocardiography for left ventricular hypertrophy. Results – Mean maximal BP during submaximal bicycle exercise test is higher than mean maximal BP during submaximal treadmill exercise test (systolic BP 177,12mmHg vs. 160.63mmHg, p<0.05 and diastolic BP 92.24mmHg vs. 86.59mmHg, p <0.05). Weight and BMI can infl uence BP response in case of bicycle testing (R2= 0,16, = 0,43, p < 0,005 respectively R2= 0,11, = 0,33, p < 0,05). Men have higher systolic (t(15) = – 1.89, p < 0.05) and diastolic (t(56) = – 2.37, p < 0.05) BP than women during exercise stress test. Conclusions – Exercise BP response in controlled hypertensive patients is infl uenced by the type of exercise stress test, gender, weight and BMI simultaneously. Maximal BP values in relation to the submaximal effort test are higher for bicycle than treadmill. In the latter case the effort of peripheral muscle groups increases vasodilatation. Keywords: arterial hypertension, exercise testing, treadmill, bicycle
INTRODUCTION
The benefi t of exercise for the cardio-vascular system is well-known1. Guidelines highlight that physically active people have healthier body and mind2. Strong scientifi c evidence demonstrates that moderate exercise decreases the cardiovascular risk factors and overall mortality3. A lot of studies have documented that physical activity can modify the prognostic of some
diseases such as ischemic heart disease, chronic kidney disease, type 2 diabetes mellitus, osteoporosis, depression and anxiety. Hypertension is one of the most studied diseases in the late 20th century. Research progress regarding the risk factors and treatment is impressive5. About 9.4 million people suffer a cardiovascular event or die because of arterial hypertension. Experts approximate this number increasing to 1.5 billion in 20256,7. Developed countries try to diminish hypertension risk by applying training programs. The goal is to present people the risks and treatments they could get. Everybody could get access to pharmacological or non-pharmacological treatments, to lessons about diet, physical exercise or about others changes of life style. It is well known that exercise training helps decrease the value of blood pressure (BP). Most of the stu- dies are about aerobic exercises because they need no special devices. How physical activity lowers systemic BP is not completely understood. A paper in 2016, explains some mechanisms of BP reduction during exer- cise8. There are four main factors that induce the rise of systemic BP: sympathetic innervation, arteriolar constriction, amplifi cation of heart contraction and increased filling pressure. They all help in delivering oxygen and nutrients to active muscles9. Depending on the type of exercise some muscle groups are used more intensively. Exercise can be dynamic or static if classified by the mechanics, and aerobic or anaerobic if classified by metabolism10. Usually, in clinical practice exercise testing can be performed mainly with two devices: treadmill and bicycle. These two assume dynamic endurance effort
with a smaller or bigger component of static effort11.
SUBJECTS AND METHODS
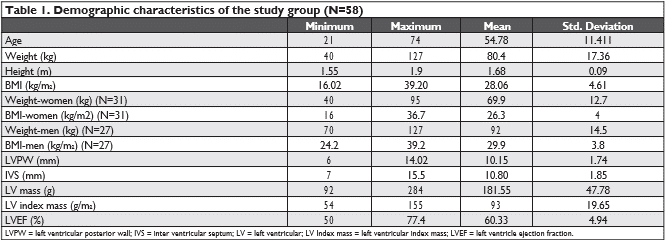
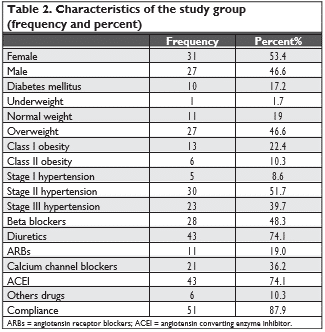
This study was performed in the Internal Medicine and Cardiology unit at “Prof. Dr. Burghele” Hospital. 58 controlled hypertensive patients (Table 1) were recruited to perform exercise stress testing: 41 using the bicycle and 17 using the treadmill. All subjects were caucasian, 27 male and 31 female with ages between 21 and 74 years old. They are hypertensive (stage one, two or three11) receiving pharmacological treatment: diuretics, calcium channel blockers, angiotensin receptor blockers, angiotensin converting enzyme inhibitors, beta blockers and centrally acting antihypertensive, in mono-therapy or in combination (Table 2). Anamnesis and clinical examination were performed for each patient. Routine blood tests, 12 lead rest electrocardiogram and transthoracic echocardiography were performed. Individuals with heart failure, secondary hypertension, electrolytes abnormalities, severe kidney disease or any other serious disorder (pulmonary, digestive, haematologic) or with contraindication for exercise stress testing were excluded from this study. After at least 2 weeks of treatment they were rechecked in a control visit. An ambulatory blood pressure monitor device (ABPM) was set up for 24 hours (General Electric Tonoport V Version). It was applied to the non-dominant arm using corresponding cuff. They received ABPM from the beginning if they al-ready had been diagnosed and treated for systemic hypertension. The recordings were processed in or-der to determine if the patient is controlled.
If the patient is controlled, he/she performed stress testing using treadmill Schiller Inter Track 8100 TMed type or ergometer bicycle Ram 660 BP, version in 7 steps. Laboratory and equipment where assessed for the standard request10. BP was automatically measu-red every 2 minutes during the test using the same device. The target heart rate was calculated by the formula (220-age (years)) x 85% for both devices. All patients achieved submaximal effort level 10. The bicycle test started with 25W for 1 minute and the workload was increased by 50W every 3 minutes. The treadmill was conducted in stages of 3 minutes each, starting with a low speed and ramp, and increa-sing progressively (Bruce protocol for treadmill). The exercise test was stopped if the target heart rate was reached, if systolic BP was >220 mmHg, if diastolic BP was >110 mmHg 10 or if any of the guideline indicati-ons of stopping occurred during the test10 . If patients did not reach target heart rate or the test was positi-ve they were excluded from the study. After the test was stopped the subjects continued to walk or pedal for 7 minutes at a low speed until the recovery stage is complete.
DATA ANALYSIS
Data was analyzed using SPSS. Categorical variables were expressed as proportions and percentages and continuous variables were expressed as means ± stan-dard deviation. Student T-test was used to compare maximal systolic and diastolic blood pressure during exercise on treadmill or on bike. For categorical vari-able Chi-square test was used. P<0.05 was consider statistically signifi cant.
RESULTS
Descriptive characteristics were established for the two groups and for all subjects. 58 controlled hyper-tensive patients were recruited to perform exercise stress testing. 41 subjects used the ergometer bicycle and 17 used the treadmill. There were 27 male and 31 female with age between 21 and 74 years old (mean age 54.5 years). Females had average weight 69.9 kg (minimal 40kg and maximal 95kg standard deviation 12. 7kg) with average body mass index (BMI) 26.3kg/ m2 (range 16kg/m2 and 36.7kg/m2, standard deviation 4 kg/m2) and males had average weight 92 kg (minimal 70 kg and maximal 127 kg, standard deviation 14.5 kg/ m2) and BMI 29.9 kg/m2 (range 24.2 kg/m2 and 39.2 kg/ m2, standard deviation 3.8 kg/m2 ). Most of them (27 patients) were overweight (Table 2).
5 subjects had fi rst stage hypertension, 30 subjects had second stage hypertension and 23 third stage hypertension according to the 2013 European Gui-delines for the management and treatment of arte-rial hypertension11. All patients received medications, monotherapy or combination of antihypertensive drugs. Most of them received diuretics and angioten-sin converting enzyme inhibitors (43 from total of 58), 28 received beta blockers, 11 angiotensin receptor blockers, 21-calcium channel blockers (amlodipine) and 6 centrally acting antihypertensive. Table 3 pre-sents the incidence of left ventricle concentric remo-deling or hypertrophy.
There was no signifi cant difference between the two groups (bike or treadmill) or between men and women. Also there was no statistically signifi cant di-fference regarding the treatment pro fi le. Mean maxi-mal systolic BP on ergometer bicycle was signifi cantly higher than mean maximal systolic BP on treadmill (177.12 vs. 160.63, p=0.011). Mean diastolic maximal BP was signifi cantly higher in the ergometer bicycle group (92.24 vs. 86.59, p=0.016) Table 4, Figure 1.
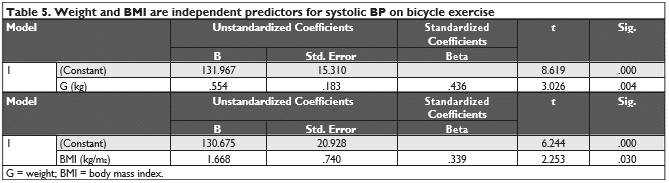
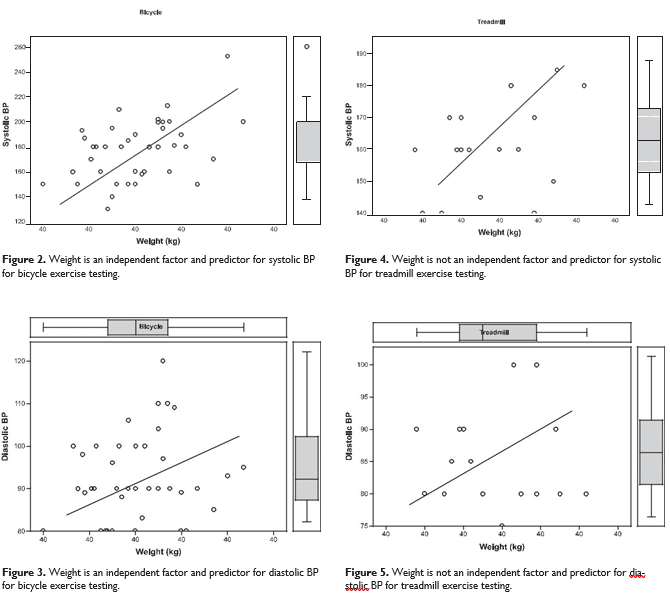
Linear regression was used to determine if weight is an independent factor and predictor for exercise blood pressure. Results show that the weight (R2= 0.16, = 0,43, p < 0,005) and BMI (R2= 0.11, = 0,33, p < 0,05) are signifi cantly independent factors and predictors for systolic BP from bicycle exercise testing (Table No 5) (Figure No 2 and 3), but not for systolic BP on treadmill (Weight: R2= 0.11, = 0.40, p > 0.10, BMI: R2= – 0,03, = 0.18, p > 0.48) (Figure 4 and 5). No signifi cant difference regarding the antihyper-tensive medication among the two groups (bike or treadmill exercise) was seen. Left ventricle mass, left ventricle mass index, hypertrophy type or left ventri-cle ejection fraction did not infl uence the BP response during the two exercise testing.
Males had higher systolic and diastolic BP values than female during exercise testing regardless of the device used. The same result was found for bicycle testing (males had higher systolic and diastolic BP). For the treadmill group results were marginally signifi – cant (maybe due to the small number of participants).
Patients with fi rst stage hypertension had lower di-astolic BP during exercise than patients with second and third stage hypertension.
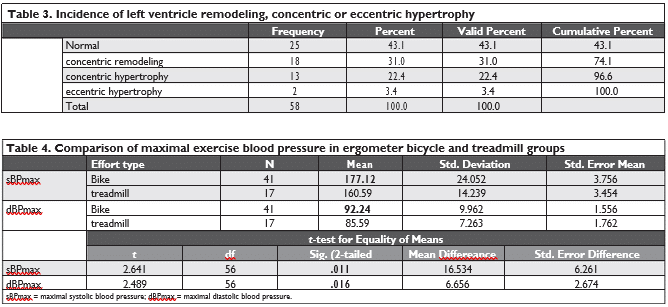
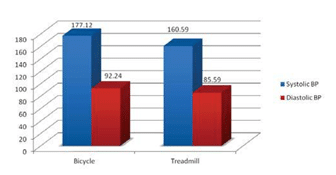
Figure 1. Comparison of maximal exercise blood pressure in ergome-ter bicycle versus treadmill patients groups, in relation with submaximal stress test (see text).
DISCUSSION
Cardiovascular response to exercise was studied extensively. Literature suggests that resting arterial blood pressure has a strong infl uence on exercise BP.
It seems that age and BMI are not very important in exercise response12.
These study results show that the patients with fi rst stage hypertension had lower diastolic BP during exercise than patients with second and third stage hypertension and men had higher systolic and diasto-lic BP during exercise stress tests than women.
The impact of exercise type (isometric or isoto-nic) on the cardiovascular system, especially BP was less studied. Exaggerated blood pressure response in normotensive patients is considered systolic blood pressure ≥210mmHg for men and ≥190mmHg for women and diastolic blood pressure ≥90mmHg for both genders10. But the same guidelines propose re-lative indication for stopping the exercise testing if systolic BP is above 250mmHg or diastolic BP above 115mmHg11. Many physicians do not agree with the-se values. They consider them exaggerated with risk for cardiovascular events. This risk would increase in hypertensive patients with subclinical organ damage. Guidelines mention that there is insuffi cient data to support this issue10.
All these cut off values are for normal BP values at rest. Can these values be used for hypertensive sub-jects who are receiving treatment and have normal ABPM values? This study tries to achieve more data about BP response to exercise in controlled hyper-tensive subjects. It suggests that the type of exercise stress test has a role in BP response. Systolic and di-astolic BP is higher for the group who used the ergometer bicycle. Active muscle involved in walking and running on treadmill are higher than in cycling. Cyclists mostly use the quadriceps muscle (a big ac-tive muscle). Subjects from treadmill group use more muscles so they produce more vasodilation than the bike group. This could explain the results of this study. Another explanation could be that it is easier to mea-sure BP on a bike. Thus the accuracy is lower for the treadmill group because of constant motion.
This study found that weight and BMI are signifi – cantly independent factors and predictors for systolic BP for bicycle exercise testing, but not for systolic BP of those tested on treadmill. Contrary, some studies show that weight is important in exercise testing on treadmill13.
In several trials the treadmill appears to be less applicable than bicycle in exercise testing. Cycle allows more accuracy and stability for electrocardiography recording and BP measurement14.
LIMITATIONS OF THE STUDY
One limitation is the small number of subjects. Even if the BP was determined automatically there may by differences of systolic and diastolic values during exercise stress tests methods (bicycle or treadmill).
CONCLUSION AND FUTURE PERSPECTIVES
Exercise stress test on bicycle respectively treadmill infl uence the BP response in different ways. Thereby maximal BP is higher during bicycle versus treadmill exercise test. The results of this study can change re-commendations for non-pharmacological treatment for hypertension. New maximal cut -off BP values should be established for hypertensive patients during different methods of exercise tests in clinical depart-ments. Especially these new maximal cut-off BP values should be used for hypertensive patients who are controlled by medication.
Further research is required for a better under-standing of exercise BP response during different stress tests in normal and hypertensive subjects.
Conflict of interest: none declared.
References
1. M. G. Schultz, “The clinical importance of exercise blood pres-sure”. Artery Res., vol. 20, p. 44, 2017.
2. K. Mikkelsena, L. Stojanovskaa, M. Polenakovicb, M. Bosevskic, and V. Apostolopoulos, “Exercise and mental health”. Acta Psychi-atr. Scand., vol. 76, no. 2, pp. 113-120, 1987.
3. P. Kokkinos and J. Myers, “Exercise and physical activity: Clinical outcomes and applications”. Circulation, vol. 122, no. 16, pp. 1637-1648, 2010.
4. D. E. R. Warburton, C. W. Nicol, and S. S. D. Bredin, “Health ben-efi ts of physical activity: the evidence”. Can. Medial Assoc. J., vol. 174, no. 6, pp. 801-809, 2006.
5. L. R. Krakoff, “Worldwide Hypertension: The Growing Threat and the Potential Opportunities”. Ann. Glob. Heal., vol. 82, no. 2,
pp. 225-226, 2016.
6. S. Y. Angell, K. M. De Cock, and T. R. Frieden, “A public health ap-proach to global management of hypertension”. Vol. 385, no. 9970,
pp. 825-827, 2016.
7. A. Chockalingam, “Impact of World Hypertension Day”. Can. J. Cardiol., vol. 23, no. 7, pp. 517-519, 2007.
8. A. Sabbahi, R. Arena, A. Elokda, and S. A. Phillips, “Exercise and Hypertension: Uncovering the Mechanisms of Vascular Control”. Prog. Cardiovasc. Dis., vol. 59, no. 3, pp. 226-234, 2016.
9. A. C. Guyton and J. E. Hall, Tratat de fi ziologie a omului, Ed a 11-a. Editura Medicala Callisto, 2007.
10. G. F. Fletcher et al., “Exercise standards for testing and training: A scientifi c statement from the American heart association”. Circu-lation, vol. 128, no. 8, pp. 873-934, 2013.
11. G. Mancia et al., “2013 ESH/ESC guidelines for the management of arterial hypertension: The Task Force for the management of arte-rial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)”. Eur. Heart J., vol. 34, no. 28, pp. 2159-2219, 2013.
12. V. Tuka, J. Rosa, M. Dedinova, and M. Matoulek, “The determi-nants of blood pressure response to exercise”. Cor Vasa, vol. 57, no. 3, pp. e163-e167, 2015.
13. R. Kisan, S. R. Kisan, O. Anitha, and S. Chandrakala, “Treadmill and Bicycle Ergometer Exercise: Cardiovascular Response com-parison”. Glob. J. Med. Res., vol. 12, no. 5, 2012.
14. K. Wielemborek-Musial, K. Szmigielska, J. Leszczynska, and A. Jegier, “Blood Pressure Response to Submaximal Exercise Test in Adults”. Biomed Res. Int., vol. 2016, 2016.
 This work is licensed under a
This work is licensed under a