Emilia Dana Baibata1, Oana Catalina Cosor1, Florin Mitu2, Mircea Iurciuc1, Silvia Mancas1
1 “Victor Babes” University of Medicine and Pharmacy,Timisoara, Romania
2 “Grigore T. Popa” University of Medicine and Pharmacy, Iasi, Romania
Background: Vascular dysfunction, including the arterial stiffness, indicates systemic vulnerability for major cardiovascular events. Identifying these changes in the vascular structure and function during preclinical stages, as well as establishing their appropriate use for risk stratification in clinically manifested disease, will bring benefits for both individuals and populations. Our study aims – To analyze the arterial function using the arteriography method in asymptomatic subjects with cardiovascular risk profile assessed using the Framingham and SCORE prediction equations. Materials and method – 35 subjects from the Cardiovascular Rehabilitation Clinic – Institute of Cardiovascular Diseases Timisoara were included in the study. They were evaluated from several perspectives: global cardiovascular risk- SCORE risk charts, Framingham risk charts; cardio-metabolic risk: traditional cardiovascular risk factors, metabolic syndrome-the IDF criteria; hemodynamic profi lesystolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MBP), pulsed pressure (PP); arterial wall stiffness: carotid femoral pulse wave velocity (PWVAo) and the systolic augmentation expressed by the Arteriography (Aix). Results – We found positive correlations between: systolic augmentative index (Aix) and pulse wave velocity (PWVAo) (p <0.001, r = 0.28), Aix and MBP (mean blood pressure) (p <0.005, r = 0.46), and PWVAo and DBP (diastolic blood pressure) (p <0.001, r = 0.62). The risk for fatal cardiovascular events in the next 10 years was signifi cantly positively correlated with the arterial stiffness: Aix and risk Score (p = 0.021). Conclusions – We appreciated the arterial function using non invasive methods and we found statistical correlations between arterial function and hemodynamic variables of the cardiovascular risk. Metabolic syndrome variables were not statistically signifi cant associated with arterial stiffness degree appreciated by Aix. We also found a statistically significant positive correlation between arterial stiffness and risk of fatal cardiovascular event over the next 10 years.
Keywords: aterosclerosis, arterial function, pulse wave velocity, pulse pressure, cardiovascular risk, arterial stiffness.
INTRODUCTION
Vascular dysfunction, including arterial stiffness and preclinical morphologic changes in the arterial vascular bed, are abnormalities indicating systemic vulnerability for cardiovascular major events. Discovering these struc tural changes and vascular function during preclinical stages, and appropriate use for risk stratification during the disease stage, brings benefi ts for both the
individuals and population1,2. The early functional disorder primarily involves the resistance vessels (small arteries, arterioles) leading over the years to the loss of elasticity of medium and large arteries (high stiffness), then to macro-vascular atherosclerotic changes and finally, to the formation of the atherosclerotic plaques2-4. In this stage of atherosclerosis, the fi rst sign of macro-
vascular atherosclerosis is represented by the decreasing of the aortic arterial wall elasticity, leading to the development of a high aortic stiffness (characteristic to the increase of PWVAo).
MATERIALS AND METHODS
Patients: In the study were included 35 patients with an accumulation of cardiovascular risk factors. They were hospitalized in the Cardiovas cular Rehabilitation Clinic Institute of Cardiovascular Diseases Timisoara in order to study their arterial function and for the assessment of the cardiovascular risk. Inclusion criteria: asymptomatic with low and high cardiovascular risk, EF >35%. Exclusion criterias: arrhythmias, valvulopathies, congenital cardiac diseases, asymptomatic with medium cardiovascular risk, EF ≤35. Clinical Evaluation: for each patient were followed:
anamnesis, family history of cardiovascular disease, quantified cardiovascular risk factors from SCORE risk pre diction equations (age, sex, systolic blood pressure, smoking, total cholesterol) or the Framingham risk charts (age, sex, total cholesterol, HDL-C, smoking, systolic blood pressure). Assessment of the absolute risk for cardiovascular events We started the evaluation of the 10-year fatal cardiovascular risk using SCORE nomogram, in accordance with Euro pean Guidelines for Cardiovascular Disease Prevention www.heartscore.org. According to SCORE risk, patients were divided into two categories: asymptomatic with low cardiovascular risk and asymptomatic with high cardiovascular risk. We used the SCORE electronic version as well in order to take into account the HDL-c, noted as Score-HDL. We rated the group of patients by calculating the 10-year risk of coronary heart disease accord ing to the Framingham model, using the interactive electronic diagram calculation: http://www.framinghamheartstudy.org/risk/ coronary. html. Cardio-metabolic risk assessment The lipid profi le analysis was performed as recommended
by guidelines of the European Society of Cardiology. The framing of the subjects in each risk category was made according to the rec ommendation of the European Society of Cardiology Guidelines. The metabolic syndrome was defi ned according to IDF criteria if they were associated with at least 3 of the 5 criteria. Hemodynamic risk assessment Based on the results of the 24h automatic recording (per formed by the BTL-08 ABPM), the analysis of the arterial blood pressure was done. Measurements were performed every 15 minutes during the day (7 am- 23 am) and every 30 minutes during the night (23-7 am). The monitoring was repeated when there were more than 30% artifacts. From the ambulatory blood pres sure monitoring protocol, we used the following parameters: 24-hour SBP, 24-hour DBP, PP 24 hours, 24 hours MAP (3). We have defi ned the following categories: normal BP <130/85, hy pertension: SBP ≥140 mmHg and / or DBP ≥90 mmHg or an tihypertensive treatment, which corresponds to an average 24- hour BP >120/80 mmHg3. Mean 24-hour pulse pressure >60 mmHg was considered pathological. Assessment of arterial function We followed the exact recommendations of the evaluation protocol using the arteriography method as described by the bibliographic references2. We analyzed the following parameters: arterial augmentation index (Aix) and aortic pulse wave velocity (PWVAo). Statistical analysis of data: data normal ity was assessed using Shapiro-Wilk test. Data were analyzed
using parametric tests-One Sample t test for comparing the mean values of two groups, and One Way ANOVA for comparing the mean values obtained in more than three groups. The testing of the association between qualitative variables was performed using Chi square test, and for testing correlations between numerical variables, we used Pearson correlation coefficient. For statistical analysis, P.A.S.W. statistics 18.0 was used.
RESULTS
We studied 35 patients, asymptomatic in terms of cardiovascular, but presenting the accumulation of wicardiovascular risk factors, hospitalized in Clinic of Cardiovascular Rehabilitation-Institute of Cardiovascular Dis eases Timisoara, of which a higher percentage (68.6%) was represented by women, the average age of the sampled patients was 49.51 (±17.19) years, 11.4% of patients had diabetes mellitus, 20% of patients had a SCORE risk ≥5%, 5.71% had a Framingham risk ≥20 and 48.57% were smokers (Figure 1,Table 1). Arterial stiffness behavior according to hemodynamic profi le of the sampled patients We have obtained a positive correlation between the aortic augmenting index and the two variables that characterize the hemodynamic profi le of SBP (p<0.003, r= 0.48) and MAP (p <0.005, r = 0.46) (Table 2).
Figure 1. The lot gender.
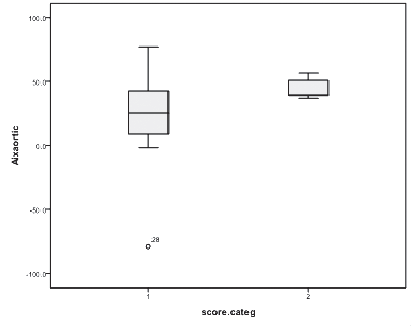
Figure 2. The Aixaortic in the risk Score categories (1-asymptomatic with low cardiovascular risk and 2-asymptomatic with high cardiovascular risk).
The correlation between arterial stiffness and risk of fatal cardiovascular event over the next 10 years For the estimation of the risk of fatal cardiovascular event in the next 10 years, we used three methods of calculation as detailed in Material and Methods section. We obtained significant differences of mean aortic Aix in the SCORE risk categories (p =0.021). We found increasing,
augmentation index (Aix) proportionally with the increasing of the risk Score, as shown in Figure 2, Table 3 and Table 4. We obtained a statistically signifi cant association relationship between Aix aortic and risk Framingham (p = 0.034, test Chi2 95% CI), but we didn’t found signifi cant differences of average Aix aortic in Framingham risk categories (p = 0.255 Test Man-Whitney 95% CI) as shown in Figure 3.
DISCUSSION
Our study demonstrates the relationship between arterial stiffness (PWVAo) and hemodynamic parameters (SBP, DBP, MAP, PP), age and risk of cardiovascular events in 10 years (SCORE risk, SCORE- HDL risk, Framingham risk). The study conducted by Hansen TW and colleagues (1) has demonstrated the necessity of measuring arterial stiffness’s (PWVAo) for asymptomatic people without cardiovascular disease, proving that the rate of aortic pulse wave propagation alone, without keeping track of the independent classical risk factors, is an effective predictor of cardiovascular mortality based on a follow-up period of 9 years6-8. In our study, we have demonstrated the existence of cor relations between arterial stiffness, hemodynamic parameters and SCORE risk. With or without being associated with the traditional risk factors, PWV represents a very important predictor of cardio vascular events9-11. The predictive value of Aix for cerebrovascular events should not be considered only in terms of hemodynamics, but also in terms of cardio-metabolic. G. Leoncini and co. have studied the association between Aix and the metabolic profi le of 156 non-diabetic, hypertensive patients, and concluded that the prevalence of increased Aix was higher in patients with metabolic syndrome12-14. Aortic PWV measurement supplies information, primarily on the properties of the aortic wall.
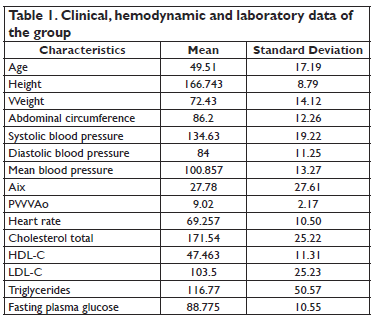

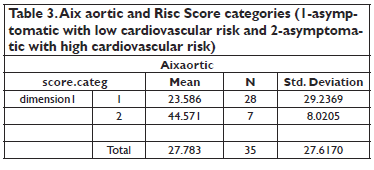
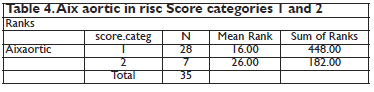
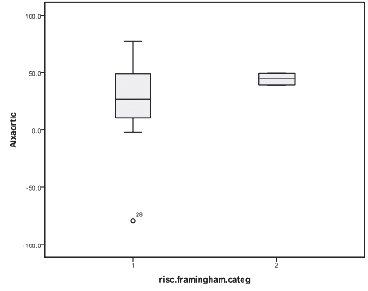
Figure 3. Aixaortic and risc Framingham categories (1-asymptomatic with low cardiovascular risk and 2-asymptomatic with high cardiovascular risk).
The more rigid and impervi ous the aortic wall is, the faster the pulse wave travels along it. We must take into ac count situations where there is an increase of the ejected blood volume in the aorta (e.g. hyper tension, tachycardia, increased cardiac output), circumstance that determines an increase in aorta diameter, therefore in creasing the parietal blood pressure, resulting in an increase in propagation velocity of wave pulse. In conclusion, aortic PWV provides a prognostic value only if it was measured in isobaric conditions, that means in normo tensive conditions9,15-17. The correlation between the arterial stiffness and the cardiovascular risk was conclusively demonstrated
in the study conducted by Guerin and co. in 2001, performed on a group of patients in end-stage kidney disease. They effectively de creased the blood pressure and followed the changes of aortic PWV in parallel. In the group that besides lowering blood pres sure, the aortic PWV was decreased as well, all patients survived the tracking period. Instead, the group in which the lowered blood pressure was not accompanied by a decrease in the aortic PWV, all patients died by the end of follow-up period of 51 months18-21. This shows, that in this second group, contrary to the first group, the increased aortic PWV was not caused by parietal tension due to hypertension, but rather by morphological ves sel lesions.
CONCLUSIONS
We assessed arterial function us ing noninvasive methods and we found statistical correlation between arterial stiffness and hemodynamic variables of cardiovascular risk, but not with metabolic profile.
We also found statistically significant positive correlation between arterial stiffness and risk of fatal cardiovascular event in the next 10 years.
It is essential to detect real individual risk, even in early reversi ble stages of atherosclerosis, when most patients are still asymp tomatic and without subjective complaints, therefore we have the
chance to favorably infl uence the process thru.
Conflict of interest: none declared.
References
1. Willum-Hansen T, Staessen JA, Torp-Pedersen C, Rasmussen S, Thijs L, Ibsen H, Jeppesen J., et al. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation, 2006; 113: 663-664.
2. Giuseppe Mancia, Robert Fagard, Krzysztof Narkiewicz, Josep Redon, Alberto Zanchetti, Michael Böhm, Thierry Christiaens, Renata- Cifkova, Guy DeBacker, Anna Dominiczak, Maurizio Galderisi, Diederick E. Grobbee, Tiny Jaarsma, Paulus Kirchhof, Sverre E. Kjeldsen, Stéphane Laurent, Athanasios J. Manolis, Peter M. Nilsson, Luis Miguel Ruilope, Roland E. Schmieder, Per Anton Sirnes, Peter Sleight, Margus Viigimaa, Bernard Waeber, Faiez Zannad, Josep Redon, Anna Dominiczak, Krzysztof Narkiewicz, Peter M. Nilsson, Michel Burnier, Margus Viigimaa, Ettore Ambrosioni, Mark Caufi eld, Antonio Coca, Michael Hecht Olsen, Roland E. Schmieder, Costas. The 2013 Guidelines for the Management of Arterial Hypertension. European Heart Journal
(2013) 34, 2159–2219 doi:10.1093/eurheartj/eht151
3. Willum-Hansen T, Staessen JA, Torp-Pedersen C, Rasmussen S, Thijs L, Ibsen H, Jeppesen J. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation, 2006; 113: 663-670.
4. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012) The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). European Heart Journal (2012) 33, 1635–1701 doi:10.1093/eurheartj/ehs092
5. O ‘Rourke MR, Brunner HR. Introduction to arterial compliance and function. J. Hypertens. Suppl., 1992; 10: 53-55.
6. Aboyans V, Criqui MH, Abraham P, Allison MA, Creager MA, Diehm C, Fowkes FG, Hiatt WR, Jonsson B, Lacroix P, et al. Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association. Circulation. 2012;126(24):2890– 909.
7. Guerin AP, Blachel J, Panniel B. Impact of aortic stiffness attenuation on survival of patients in end-stage renal failure. Circulation, 2001; 103:987-992.
8. Fowkes FG, Murray GD, Butcher I, Heald CL, Lee RJ, Chambless LE, Folsom AR, Hirsch AT, Dramaix M, deBacker G, et al. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA. 2008;300(2):197– 208.
9. The CAFÉ Investigators, for the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) Investigators. Differential impact of blood pressure- lowering drugs on central aortic pressure and clinical outcomes. Principal results of the Conduit Artery Function Evaluation (CAFÉ) Study. Circulation. 2006; 113:
10. Redheuil A., Yu W.C., Wu C.O.; Reduced ascending aortic strain and distensibility: earliest manifestations of vascular aging in humans. Hypertension. 55 2010:319-326.
11. Papaioannou TG, Karageorgopoulou TD, Sergentanis TN, et al. Accuracy of commercial devices and methods for noninvasive estimation of aortic systolic blood pressure a systematic review and metaanalysis of invasive validation studies. J Hypertens. 2016 Apr 28. [Epub ahead of print]
12. Malayeri A.A., Natori S., Bahrami H.; Relation of aortic wall thick ness and distensibility to cardiovascular risk factors (from the Multi-Ethnic Study of Atherosclerosis [MESA]). Am J Cardiol. 102 2008: 491- 496.
13. Nelson M.R., Ste panek J., Cevette M., Covalciuc M., Hurst R.T., Tajik A.J.; Noninvasive measurement of central vascular pressures with arterial tonometry: clinical revival of the pulse pressure waveform?. Mayo Clin Proc. 85 2010:460-472.
14. Williams B, Lacy PS, Thom SM, Cruickshank K, et al. The CAFE Investigators for the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) Investigators, CAFE Steering Committee and Writing Committee. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the conduit artery function evaluation (CAFE) Study. Circulation, 2006; 113: 1213-25.
15. O ‘Rourke MR, Staessen JA, Vlachopoulos C, et al. Clinical ap plica tions of arterial stiffness: defi nitions and reference values. Am. J. Hypertens., 2002; 15: 426-44.
16. McEniery C.M., Spratt M., Munnery M.; An analysis of prospective risk factors for aortic stiffness in men: 20-year follow-up from the Caerphilly prospective study. Hypertension. 56 2010:36-43.
17. Bramwell J.C., Hill A.V., McSwiney B.A.; The velocity of the pulse wave in man in relation to age as measured by the hot-wire sphygmograph. Heart. 10 1923:233-255.
18. Van Bortel LM, Duprez D, Starmans-Kool MJ, Safar ME, Giannat tasio C, Cockcroft J, et al. Clinical applications of arterial stiffness, Task Force III: recommendations for user procedures. Am. J. Hypertens., 2002; 15: 445-452.
19. Safar ME, Blacher J, Mourad JJ, London GM. Stiffness of carotid artery wall material and blood pressure in humans: application to antihypertensive therapy and stroke prevention. Stroke 2000; 31:782–790
20. Roman MJ, Devereux RB, Kizer JR, Lee ET, Galloway JM, Ali T, et al. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure; The Strong Heart Study. Hypertension, 2007; 50:197.
21. Korhonen PE, Seppala T, Kautiainen H, Jarvenpaa S, Aarnio PT, Kivela SL. Ankle-brachial index and health-related quality of life. Eur J Prev Cardiol. 2012;19(5):901–7.
22. Mattace-Raso FUS, van der Cammen TJM, Hofman A, van Popele NM, Bos ML, Schalekamp MADH, Asmar A, Reneman RS, Hoeks APG, Breteler MMB, Witteman JCM. Arterial stiffness and risk of coronary heart disease and stroke: The Rotterdam Study. Circulation. 2006; 113: 657–663.
23. Pauca AL, O’Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension. 2001; 38: 932–937.
24. www.heartscore.org
25. http://www.framinghamheartstudy.org
 This work is licensed under a
This work is licensed under a