Marius Rac-Albu1, Mihaela Sălăgean2, Mădălina Găvănescu2, Isabella Oprea2, Marian Croitoru2
1 „Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
2 „Prof. Dr. C.C. Iliescu” Emergency Institute for Cardiovascular Diseases, Bucharest, Romania
Contact address:
Marius Rac-Albu, MD
„Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
racalbu@yahoo.com
The ankle-brachial index (ABI) is an efficient tool for objectively documenting the presence of lower-extremity peripheral arterial disease (PAD)1,2. Additionally, the ABI has been shown to predict mortality and adverse cardiovascular events independent of traditional CV risk factors.
We present the case of a male patient, aged 60 years with multiple cardiovascular risk factors: smoker, hypertensive, dyslipidemic, with history of intermittent claudication for several years and the gradual decline of the walk perimeter which is hospitalized for worsening of intermittent claudication at 30 m, accentuated at the level of right lower limb. The patient associated vasospastic angina, stable angina episodes of exertion.
Clinic at admission – blood pressure 160/90 mmHg, heart rate 96/min, rhythmic heart sounds without heart or carotid murmurs, without pulmonary rales, right lower limb with pale skin and cold at the level of the leg and the distal half of the leg, sensitivity and motility preserved, absent femoral pulse. Left lower limb shows warm skin, normal colored, sensitivity and motility preserved, femoral pulse present, absent distally.
ECG preoperative – sinus rhythm, 61/min, QRS axis +40 degrees, no significant changes of ST-T segment.
Preoperative coronary angiography – showed permeable coronary artery.
For appreciation of arterial occlusive disease severity, it was performed preoperative ankle-brachial index (ABI); its values were: ABI = 0 to the right lower limb and ABI = 0.58 in the left lower limb.
Lower limb arteriography was performed with left femoral approach and it showed: terminal aorta (Ao) with plaques without significant stenosis. Right arterial axis with external iliac artery (EIA) occlusion and the common femoral artery (CFA) reloading, also diffusely infiltrated vessel, superficial femoral artery (SFA) occlusion from its origin, reload of the proximal popliteal artery, permeable arterial leg trunks.
Left arterial axis: external iliac artery and common femoral artery with plaques realizing a partial stenotic lesion till 50-60%. SFA – diffuse infiltration vessel with 80% stenosis, proximal popliteal artery and leg arterial trunks being permeable.
It was decided and made right CFA and left SFA endarterectomy at origin and the first portion, lower limb reconstruction by aorto-common bifemural bypass grafting using 16/8mm Y-shaped-Dacron-Prosthesis. Postoperative evolution was favorable, with warm lower limbs, good arterial circulation and supple postoperative plagues, without local inflammatory phenomena, good tolerance while walking. It was performed early postoperative ankle-brachial index with increasing values from preoperative evaluation: ABI = 0.43 to the right lower limb and ABI = 0.69 in the left lower limb.
The ankle-brachial index is the systolic pressure in the ankle (either the dorsalis pedis or the posterior tibial artery, whichever has the higher pressure) divided by the systolic pressure in the arm (either the left or right, whichever is higher). The lower of the two values obtained (left and right) is the patient’s overall ankle-brachial index.
Its advantage is the simplicity in which it can be determined and that it is a noninvasive exploration. Normal cut-off values chosen for most studies, and those accepted by the guidelines of cardiology societies are between 0.9 and 1.4.
An abnormal ankle-brachial index below 0.9 is a powerful independent marker of cardiovascular risk. There is an inverse correlation between the ABI, non-fatal cardiac events (myocardial infarction, stroke, exacerbated heart failure) and cardiovascular mortality, increased risk is nonlinear, patients with very low ABI (<0.3) having an additional risk significantly higher3-6. Also, the continuous decrease in ABI is an independent prognostic factor7.
In general, patients with low ABI are predominantly male, older, former smokers and were more frequent alterations in renal function. From the risk factors associated with PAD, hypertension and diabetes are most correlated with low ABI8.
In conclusion, we have presented the case of a patient with multiple risk factors, known with vasospastic angina presenting for worsening claudication index in the aorto-iliac peripheral disease. He associated aggravated angina but without ECG changes or enzyme dynamics, preoperative coronary angiography showing coronary arteries permeable. Post aorto-common bifemural bypass grafting we achieved a good improvement in walking tolerance and ankle-arm index.
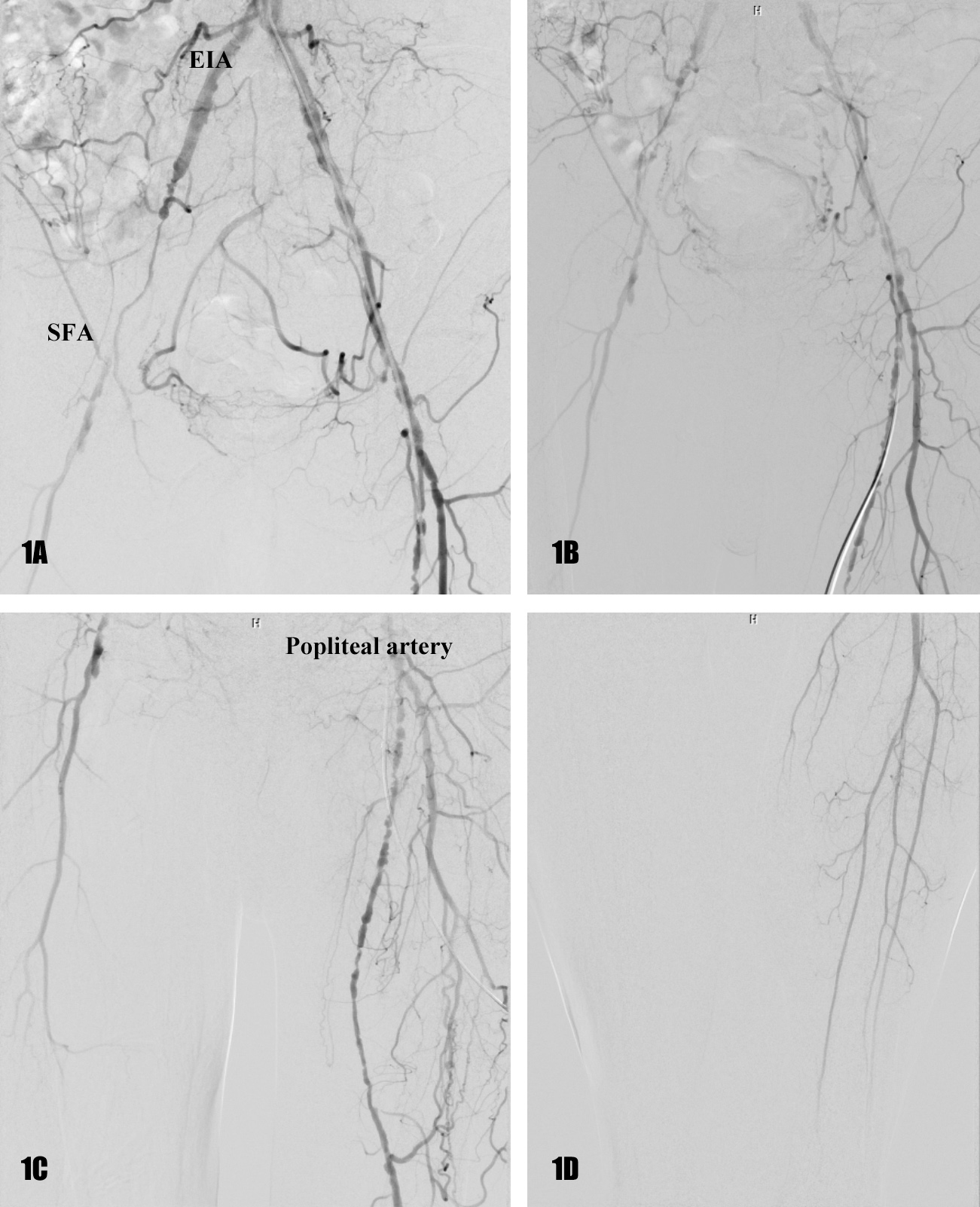
Figure 1. Right arterial axis: EIA occlusion and the CFA reloading, SFA occlusion from its origin, reload of the proximal popliteal artery. 1B. Left arterial axis: EIA and CFA with serial stenosis 50-60%, SFA – diffuse infiltration vessel with 80% stenosis. 1C. Proximal popliteal artery and leg arterial trunks – diffuse and severe atheromatous infiltration, but permeable. 1D. Tardiv reload of the proximal popliteal artery, permeable arterial leg trunks.
Conflicts of interests: none declared.
References
1. Lange SF, Trampisch HJ, Pittrow D, Darius H, Mahn M, Allenberg JR. Profound influence of different methods for determination of the ankle brachial index on the prevalence estimate of peripheral arterial disease. BMC Public Health. 2007;7:147.
2. Shanmugasundaram M, Ram VK, Luft UC, Szerlip M, Alpert JS. Peripheral arterial disease–what do we need to know?. Clin Cardiol. Jun 29 2011.
3. Leng GC, Fowkes FG, Lee AJ – Use of ankle brachial pressure index to predict cardiovascular events and death: a cohort study. BMJ 1996;313:1440-44.
4. Hooi JD, Stoffers HE, Kester AD, van Ree JW – Peripheral arterial occlusive disease: prognostic value of signs, symptomes and ankle brachial pressure index. Med Decis Making 2002;22:99-107.
5. Diehm C, Lange S, Darius Het al – Association of low ankle brachial index with high mortality in primary care. Eur Heart J 2006;27:1743-49.
6. McDermott MM, Feinglass J, Slavensky R – The ankle-brachial index as a predictor of survival in pacients with peripheral vascular disease. J Gen Intern Med 1994;9:445-45.
7. Criqui MH, Ninomiya JK, Wingard DL – Progression of peripheral aretrial disease predicts cardiovascular disease morbidity and mortality. JACC-RO 2009;1:29-36.
8. Barbara V. Howard, Elisa T. Lee – Rising Tide of Cardiovascular Disease in American Indians: The Strong Heart Study, Circulation 1999; 99:2389-2395.
 This work is licensed under a
This work is licensed under a