Irina Costache1, A. Cozma1, L. Stoica2, A. O. Petriş1
Article received on the 25th February 2012. Article accepted on the 4th May 2012.
1 1st Medical Cardiology Clinic, University of Medicine and Pharmacy “Gr. T. Popa” Iaşi, “St. Spiridon” Hospital Iaşi, Romania
2 Department of Cardio-Vascular Surgery, Institute for Cardio-Vascular Diseases Iaşi
Dr. Antoniu Octavian Petriş, 1st Medical Cardiology Clinic, University of Medicine and Pharmacy “Gr. T. Popa” Iaşi, “St. Spiridon” Hospital Iaşi, Romania.
E-mail: antoniupetris@yahoo.com
Abstract: Left atrial myxoma is one of the most common tumors of the heart, with a variety of nonspecific clinical signs and symptoms that often masquerade as many other cardiovascular or systemic diseases. We report a case of left atrial myxoma in a 73 year-old woman who initially presented with dyspneea on minimal exertion. Following the diagnosis, based on 2-D transthoracic and transesophageal echocardiography, the patient was refered to surgery for resection of the tumor – a left atrial myxoma – which was successfully removed under general anaesthesia and cardiopulmonary bypass.
Keywords: left atrial myxoma, dyspnea, echocardiography, resection
Case Study
A 73 year-old woman was admitted to the hospital because of dyspnea on minimal exertion. The patient had several cardiovascular risk factors, such as 20-year history of hypertension, high levels of cholesterol, obesity and diabetes mellitus type I treated with insulin. Recently, the patient complained about dyspnea on minimal exertion and palpitations and for a while was considered to have respiratory failure and treated according to this diagnosis. Clinical examination revealed 2nd degree obesity, sinus rythm with 3-4 premature beats per minute and a diastolic murmur at the left lower sternal border. The blood pressure was normal and the electrocardiogram indicated sinus rythm with ventricular ectopic beats and no significant ST segment or T wave changes. Chest X-ray showed enlargement of the left ventricle silhouette. Two-dimensional transthoracic echocardiography (TTE) identified an echodense mass within the left atrium (40/52 mm), protruding accross the mitral valve during diastole (Figure 1) and attached to the interatrial septum with a thin stalk. The left atrium diameters were 52/59 mm and left ventricle end-diastolic diameter was normal. The mitral annulus presented a small calcification and a mild mitral regurgitation. Doppler echocardiography revealed a peak pressure gradient through the mitral valve of 29 mmHg and a mean gradient of 19 mmHg, corresponding to a severe “relative”, „functional” mitral stenosis.

Figure 1. Transthoracic echocardiography (parasternal long-axis view) showed a huge left atrial mass (5,3 cm×4 cm) attached to the atrial septum protruding into the left ventricle during diastole.
Left ventricle ejection fraction was normal. Right ventricle and right atrium were enlarged (RA = 50/58 mm). Systolic pulmonary pressure was remarkably high (83 mmHg) as calculated using the peak pressure gradient of tricuspid regurgitation and the estimated right atrial pressure based on the diameter and respiratory variation of the inferior vena cava. Transesophageal echo-
cardiography (TEE), the most sensitive method for the diagnosis of intracardiac masses, confirmed the presence of an echodense, non homogenous mass attached to the interatrial septum (Figure 2, Panel A and B).

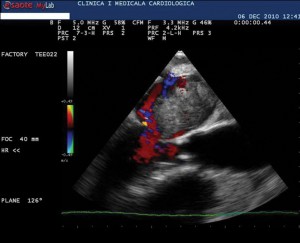
Figure 2. Two-dimensional transesophageal echocardiographic image, mid-esophageal view at: A. 126 degree demonstrates the large atrial mass (M) protruding into the left ventricle during diastole and B. 126 degree, showing a large (5 cm×3.5 cm), ovoid and heterogeneous mass (M) in the left atrium surronded by the color Dopller flow.
The patient was refered to Cardiovascular Surgery Department in order to continue the investigations and for treatment. The patient was operated under general anesthesia. TEE was used before and after extracorporeal circulation (ECC) to localize the tumor, to verify the mitral valve function and to control the presence of air in the heart cavities and the ventricular function. The tumor occupied the entire volume of the left atrium and almost blocked the mitral valve and, despite this, there was no mitral regurgitation. The ECC was established by means of an ascending aorta cannula and by two caval cannulas. The heart was arrested with 1000 ml cold blood hyperpotassemic antegrade cardioplegia injected in the aortic root. The arresting cardiac time was 32 minutes. The left atrium was open by the interatrial groove. The tumor was exposed and resected piece by piece because of it`s big size and friability (Figure 3).

Figure 3. The large atrial mass after surgical excision. Histopathology exam confirm the diagnosis of myxoma.
The tumor had a pedicle inserted on the interatrial septum. The pedicle was resected and the small atrial septal defect was directly sutured. The mitral valve was dilated, with supple leaflets; moreover, with surprise, a major regurgitation was detected after saline injection. Mitral annuloplasty was done using a 28 Edwards Cosgrove annular band with trivial residual regurgitation. Aorta was unclamped and the heart restarts promptly its activity in sinus rhythm. The ECC was stopped under inotropic support. The anatomo-pathological exam confirmed that the tumor was a myxoma. At the follow up, 6 weeks after the operation, the patient was doing well and an echocardiographic Doppler examination showed a drop of the systolic pulmonary artery pressure at 43 mmHg.
Discussion
Myxomas are the most common primary benign tumors of the heart with an incidence of 0.5 per million populations1,6. Between 75-80% of primary tumors are benign and about 50% of benign tumours are myxomas. They occur twice as much in females than in males and the mean year of detection is 55 years3. Commonly, myxomas derive from the left atrium but 25% may arise in the right atrium or even in the ventricles7. Most cases are sporadic, but up to 10% are familial and their transmittance appears to be autosomal dominant4. Usually, symptoms are non-specific and early diagnosis is rather difficult. Clinically myxomas are characterized by Goodwin’s triad: embolisation, obstruction of blood flow and constitutional symptoms such as fever and weight loss1-5. A sizeable number of patients (17 to 59%) with myxoma present clinically with an embolic event, usually in the cerebral territory9. Obstruction of blood flow can cause heart failure or syncope in 41-79% of cases. Left ventricular inflow tract obstruction because of the myxoma can mimic a mitral stenosis and can be a cause of pulmonary hypertension and congestive heart failure2. Common systemic symptoms are: fever, malaise, weight loss, fatigue, aneamia, elevated erythrocyte sedimentation rate (ESR). Both symptoms and signs resolve immediately after surgery and seems to be due by the releasing of inflammatory mediators from tumour cells1,2. Myxomas are of two types: one with round, nonmobile surface and other polypoid type with irregular surface, mobile with an increased risk of embolisation2,11. Surgical removal is the treatement of choice for myxomas. The site of the attachement should be resected with clear margin, even if that is followed by the artificial creation of an atrial septal defect that needs to be closed by a pericardial patch4,7-11. The reccurence of myxomas has been reported to be less than 2%, thus, follow up is important especially for the detection of recurrent myxomas and is easily done by clinical examination combined with 2D echocardiography4. As seen in this case, atrial myxomas may develop into giant masses without producing major symptoms which may develop late in the course of tumour life and be either vague or nonspecific. In elderly patients presenting with dyspnea but no pulmonary disease, cardiac problems must be considered as the cause of pulmonary symptoms and complaints. Echocardiography, thus in these patients as well, proves to be very useful for detecting cardiac causes for dyspnoea12.
Conflict of interests: none declared
References
1. Mac Gowan SW, Sidhy P, AhemeT şi col. Atrial myxoma: national incidence diagnosis and surgical management. Isr J Med Sci 1993; 162: 223-26.
2. Pradhan B, Acharya SP. A Case of atrial myxoma: anaesthetic management. Kathmandu University Medical Journal 2006; 15: 349-353.
3. Fang BR, Chiang CW, Hung JS şi col. Cardiac myxoma – clinical experience in 24 patients. Int J Cardiol 1990; 29: 335-341.
4. Gaspar M, Laufer G, Antretter H şi col. Mixomul cardiac – spectrul clinic variat care întîrzie diagnosticul. TMJ 2002; 2: 63-65.
5. Reynen K. Cardiac myxomas. N Engl J Med 1995; 14: 1610-7.
6. Castells E, Ferran V, Octavio F şi col. Cardiac myxomas: surgical treatement, long term results and recurrence. J Cardiovasc Surg 1993; 34: 49-53.
7. Centofanti P, Di Rosa E, Deorsola L şi col. Primary cardiac tumors: early and late results of surgical treatement in 91 patients. Ann Thorac Surg 1999; 68: 1236-41.
8. Panagiotu M, Nikolaos D, Panagopoulos D, Panagiota Ravazoula, Loukas Kaklamanis and Efstratios N Koletsis. Large asymtomatic Left Atrial Myxoma with ossification: case report. Journal of Cardiothoracic Surgery 2008; 3:19.
9. Meng Q, Lai H, Lima J, Tong W, Qian Y, Lai S şi col. Echocardiographic and pathologic characteristics of primary cardiac tumors: a study of 149 cases. Int J Cardiol 2002; 84: 69-75.
10. Bhan A, Mehrotra R, Choudhary S şi col. Surgical experience with intracardiac myxomas: long-term follow up. Ann Thorac Surg 1998; 66: 810-3.
11. Ha JW, Kang WC, Chung N şi col. Echocardiographic and morphological characteristics of left atrial myxoma and their relation to systemic embolisation. Am J Cardiol 1999; 83: 1579-82.
12. Mustafa B, Erol A. Giant left atrial myxoma causing mitral valve obstruction and pulmonary hypertension. Can J Surg 2008; 51: 97-98.
 This work is licensed under a
This work is licensed under a