Daniela I. Anghelina2, Emanuel Stoica2, Radu Stavaru2, Lucian Zarma2, Carmen Ginghina1,2
1 ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
2 ”Prof. Dr. C. C. Iliescu” Emergency Institute for Cardiovascular Diseases, Bucharest, Romania.
Abstract: Stress cardiomyopathy (also called apical ballooning syndrome, Takotsubo cardiomyopathy (TCM), broken heart syndrome, and stress-induced cardiomyopathy) is a syndrome characterized by transient regional systolic dysfunction of the left ventricle, mimicking myocardial infarction, but in the absence of angiographic evidence of obstructive coronary artery
disease or acute plaque rupture1.
Keywords: stress, ST segment elevation, normal coronary arteries
A 54-year-old woman presented to the emergency department with acute retrosternal chest pain, witch starded 3 hours ago, after an emotional stress (arguing with her husband). She had no history of angina symptoms and no conventional cardiovascular risk factors. In 2012 she had a posttraumatic sternal fracture. On presentation, the patient was hemodynamically stable, BP=130/70 mmHg, HR=100 beats/min, the oxygen saturation was 99%. Physical examination revealed a grade III/VI systolic murmur at the apex of the heart, without radiation. The electrocardiogram showed diffuse ST-segment elevations with biphasic T-wave in the precordial leads (V2-V6), also in the infero- postero- lateral leads (DI,DII, DIII, aVF, V7-V9). The QTc interval was prolonged-616 msec (Figure 1). The serum cardiac troponin level was elevated while creatine kinase level was normal (TnI=0,98 ng/ml, CK=124 U/L and CK-MB= 25 U/L). Also the level of brain natriuretic peptide (BNP) was increased (1016 pg/ml). The inflammatory markers, renal and liver function were in the normal range. The LDL cholesterol level was 85 mg/dl and the glycemia was 123 mg/dl. The transthoracic echocardiography revealed global akinesia of the mid and apical left ventricular segments with the hyperkinesia of the basal walls. There was no
obstruction of the left ventricular outfl ow tract. The overall left ventricular ejection fraction was estimated at 35% and the mitral regurgitation was mild. The pacient had spontaneous contrast in LV but no apical thrombus was detected. A presumptive diagnosis of TakoTsubo cardiomyopathy (TCM) could be made based on the echocardiographic fi ndings associated with the clinical manifestation and the electrocardiographic changes (the ECG and the regional wall-motion abnormalities extended beyond a single epicardial vascular distribution). However it was mandatory to rule out a myocardial infarction.
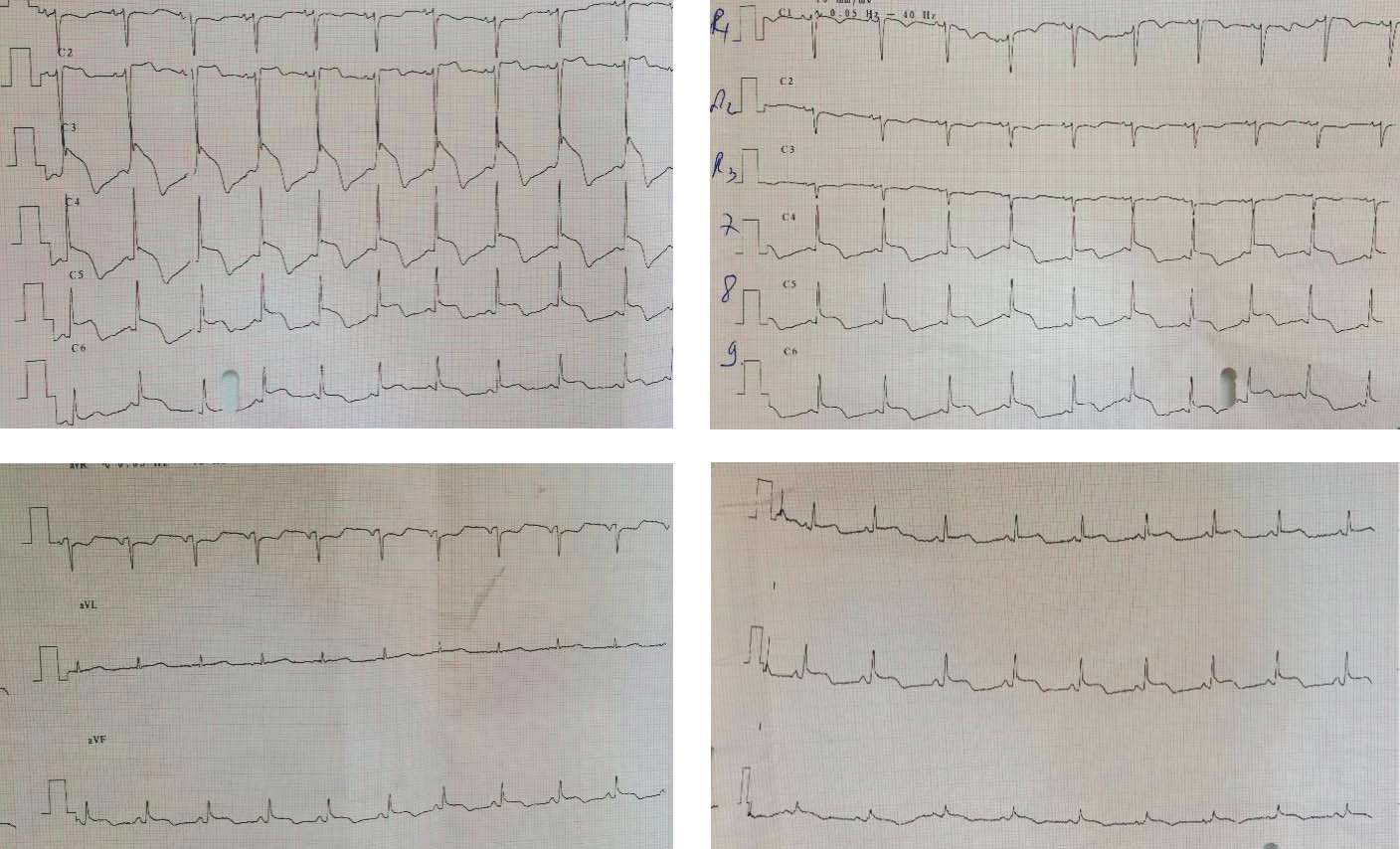
Figure 1. ECG- Diffuse ST-segment elevations with biphasic T-waves (leads V2-V6, DI, DII, DIII, aVF, V7-V9). QTc= 616 msec.
The patient was transferred to cardiac catheterisation laboratory. The coronary angiography demonstrated normal epicardial coronary arteries (Figure 2).
The left ventriculogram during systole showed mid and apical left ventricular ballooning, with vigorous contraction of the basal segments (as seen in Takotsubo cardiomyopathy). It also revealed an apical thrombus (Figure 3). The patient was initially treated as having acute coronary syndrome. She received dual antiplatelet therapy (250 mg of aspirin and 600 mg of clopidogrel) and
70 UI/kg of unfractionated heparin during PCI. In the cardiac intensive care unit, she was treated with aspirin (75 mg), betablockers (metoprolol 100 mg), angiotensin-converting enzyme inhibitors- ACE (enalapril 2,5 mg bid), loop diuretic (furosemide 40 mg), mineralocorticoid receptor antagonists (spironolactone 25 mg), statins (atorvastatin 80 mg).
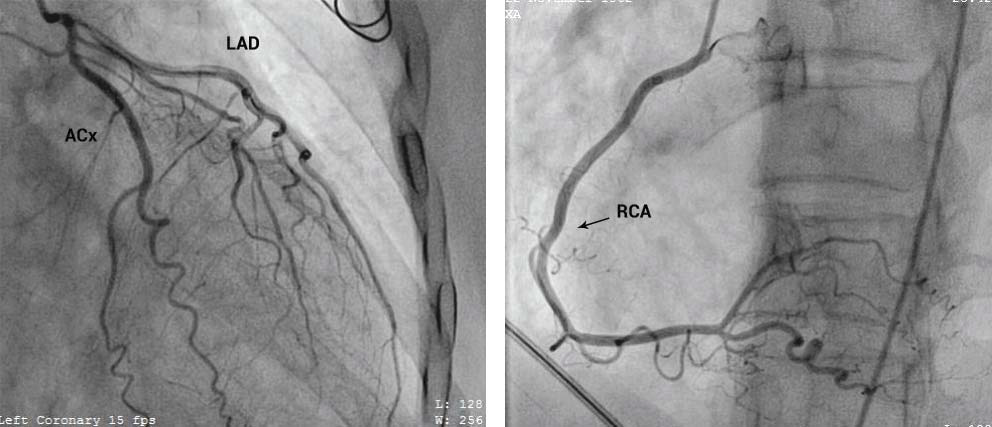
Figure 2. Coronary angiography – normal anterior descending coronary artery (LAD), circumfl ex artery (ACx) and right coronary artery (RCA).
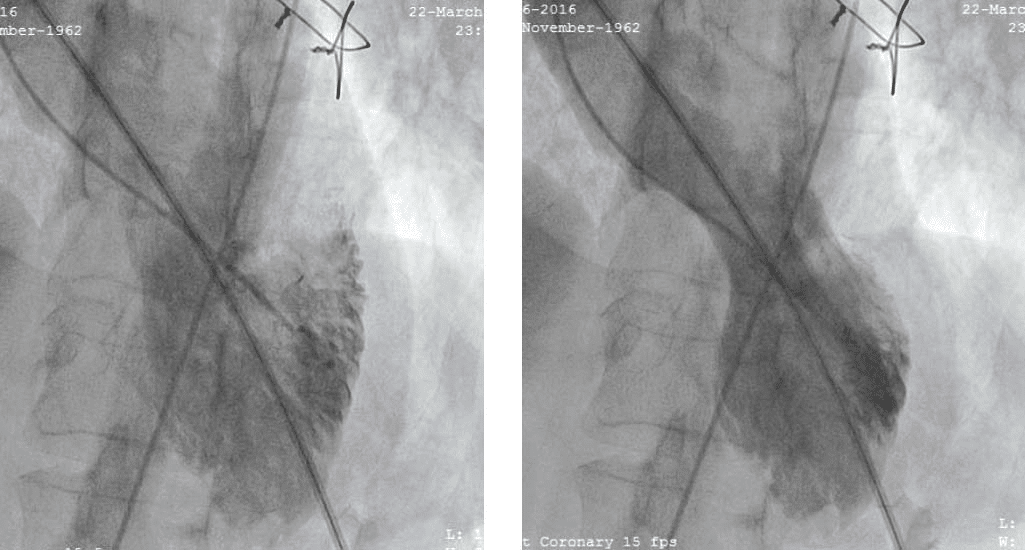
Figure 3. Left ventriculogram during systole -> mid and apical left ventricular ballooning, hyperkinesia of the basal segments. Apical thrombus (red arrow, red circle). Sternum sutures (blue arrow).
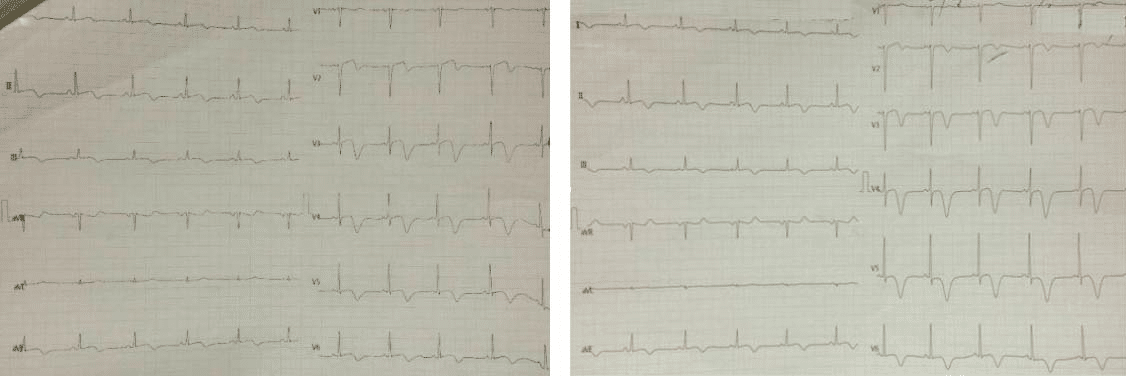
Figure 4. ECG- resolution of ST-segment elevation; difusse and deep inverted T waves. QTc = 579 msec (right fi gure).
Because of the apical left ventricular thrombus she needed anticoagulant therapy- 2 mg of acenocoumarol (together with enoxaparin 1 mg/kg subcut every 12 hours until the international normalized ratio (INR) was in the target range (2-3)). During hospitalization the patient had accused no angina or mild exertional dyspnea. The subsequent electrocardiograms showed the resolution of ST segment elevation followed by the development of diffuse, deep, inverted T waves. The QTc interval was maintained prolonged (fi gure 4). The echocardiogram showed improving LV function (LVEF= 40%) with partial resolution of the wall-motion abnormalities until discharge. The treatment recommended during next evaluation (after a mounth) was oral anticoagulant (acenocoumarol 17 mg per week- dose adjusted based on results of the INR (target INR 2-3)), betablockers (metoprolol 100 mg), ACE (enalapril 2,5 mg bid), mineralocorticoid receptor inhibitors (spironolactone 25 mg) and low dose of loop diuretic (furosemid 20 mg).
DISCUSSIONS
Takotsubo cardiomyopathy is a transient cardiac syndrome that involves left ventricular apical akinesis and mimics acute coronary syndrome. It was first described in Japan in 1990 by Sato et al. Patients often present with chest pain, have ST-segment elevation on electro cardiogram and elevated cardiac enzyme levels-abnormalities consistent with a myocardial infarction2. Left ventricular apical ballooning and no significant coronary artery stenosis are found on the coronary angiography. The pathogenesis of this disorder is not well understood. Postulated mechanisms include catecholamine excess, coronary artery spasm and microvascular dysfunction3. In Takotsubo cardiomyopathy the ECG has a typical evolution. The resolution of ST segment elevation is
followed by the appearance of diffuse and deep inverted T waves. Q waves are rare and ussualy transient. QTc interval prolongation is almost universally reported. Some autors have suggested a four phases evolution: initial ST elevation followed by transient T waves inversion (days 1-3), then T-waves recovery (days 2-6) followed by giant T-waves inversion associated with QT prolongation, witch persisted for several months. This ECG evolution seem to be helpful to differentiate myocardial infarction from TCM, but any of this ECG pattern may be seen in coronary arteries disease. The modifi ed Mayo Clinic criteria for diagnosis of TCM can be applied to a patient at the time of presentation and must contain all 4 aspects4: Transient hypokinesis, dyskinesis, or akinesis of the left ventricular midsegments, with or without apical involvement; the regional wall-motion abnormalities extend beyond a single epicardial vascular distribution, and a stressful trigger is often, but not always, present. Absence of obstructive coronary disease or angiographic evidence of acute plaque rupture. New electrocardiographic abnormalities (either
ST-segment elevation and/or T-wave inversion) or modest elevation in cardiac troponin level. Absence of pheochromocytoma or myocarditis4. There are no clear recommandations for treating
TakoTsubo cardiomyopathy. Because it mimics acute coronary syndrome, the patient should be treated as having acute coronary syndrome and the coronary angiography should be performed.
Because of the left ventricular systolic dysfunction, long-term management of this patients should include -blockers and ACE inhibitors. After LV function normalizes, physicians may consider discontinuation of these drugs. They do not prevent the disease recurrences and not improve survival rate6. It’s also important to alleviate any physical or emotional stress that may have played a role in triggering the disorder. Although there were no elements to support clinical diagnosis (severe arterial hypertension and the classical triade- headaches, palpitations, diaphoresis),
pheochromocytoma was not ruled out (plasma/urinary metanephrine testing were not available in the hospital). Also a cardiac resonance imaging was not available to rule out myocarditis. However, the TCM was strongly suggested by the associations between: (1) symptoms triggered by an emotional stress; (2) symptoms (chest pain) and ECG fi ndings suggestive of acute coronary syndrome but with normal coronary arteries on angiography; (3) echocardiographic demonstration of LV dysfunction with preserved function at the base and akinezia of all the other segments;
(4) the left ventriculogram demonstration of mid and apical left ventricular ballooning during systole and (5) improving LV function with partial resolution of the wall-motion abnormalities until discharge. Conflict of interests: none declared.
References:
1. Sato H, Taiteishi H, Uchida T. Takotsubo-type cardiomyopathy due to multivessel spasm. In: Clinical aspect of myocardial injury: From ischemia to heart failure, Kodama K, Haze K, Hon M (Eds), Kagakuhyouronsha, Tokyo 1990. p.5
2. Sato H, Tateishi H, Uchida T, et al. Clinical Aspect of Myocardial Injury: From Ischaemia to Heart Failure. Tokyo: Kagakuhyouronsya; 1990. 56-64.
3. Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med 2005; 352:539.
4. Kawai S, Kitabatake A, Tomoike H. Guidelines for diagnosis of takotsubo (ampulla) cardiomyopathy. Circ J. 2007 Jun. 71(6):990-2.
5. Eric B Tomich, DO; Chief Editor: Erik D Schraga, MD, Takotsubo Cardiomyopathy, http://emedicine.medscape.com/article/1513631-overview
6. Kazuo Komamura, Miho Fukui, Toshihiro Iwasaku, Shinichi Hirotani, and Tohru Masuyama, Takotsubo cardiomyopathy: Pathophysiology, diagnosis and treatment, World J Cardiol. 2014 Jul 26; 6(7): 602–609
 This work is licensed under a
This work is licensed under a