Adrian Ionescu1
1 Department of Cardiology, Morriston Regional Cardiac Centre, Morriston, UK
CASE REPORT
An 82-year-old woman had a mechanical fall resulting in a hip fracture. The paramedic crew in attendance recorded a 12-lead ECG as a matter of routine; it was normal. During transport to the hospital the patient experienced nausea and vomiting and became briefl y unresponsive. A repeat ECG demonstrated ST-segment elevation in leads V2- V6. The patient denied chest pain at any stage. She was brought straight to the cath lab for primary PCI. On arrival she was pale, slightly obtunded (she had received 5mg of iv Diamorphine) and her ECG showed partial resolution of the ST-segment elevation. She continued to deny chest pain. Invasive arterial pressure was 118/74 mmHg. Her only medical history was of systemic arterial hypertension for which she was taking Bendrofulazide and Enalapril. She was fail and had limited mobility due to arthritis. We performed coronary angiography via the right radial approach using 6F catheters. The epicardial coronaries were large and tortuous (in keeping with a history of systemic arterial hypertension) and were unobstructed; the RCA was dominant. There was mild pressure damping in the left main stem the ostium, which appeared stenosed (Figure 1). An IVUS examination of the LMS demonstrated an MLA at the level of the ostium of 7.6mm2 (Figure 2), clearly above any of the cut-offs previously described Figure 1. for significant LMS stenosis. LV angiography (Figure 3) revealed severe LV impairment, LVEF ~25%, and extensive apical akinesia with hyperkinetic contraction of the basal LV segments, an appearance typical for stress cardiomyopathy (TakoTsubo). The patient was treated with diuretics, ACE-I, beta-blockers and made an uneventful recovery. The orthopaedic diagnosis was that of fracture of the leftsided pubic ramus, with a sizable haematoma (which explained the initial pallor; Hb had dropped to 8.7g/L). The LMS is a notoriously difficult area of the coronary tree to evaluate by angiography alone and often requires additional interrogation by FFR or intravascular imaging1 . When FFR <0.8 was used as the gold standard, inter-observer agreement for ‘eye-balling’ of the severity of LMS diameter stenosis was only 52%2 . IVUS cutoffs for LMS diameter stenoses are still debated, but no contemporary data identify cutoffs above 7.5 mm2 ; in fact when FFR is used as the gold standard, a much lower cutoff (4.9 mm2 ) has been proposed3 although it has not been widely validated outside South-East Asia. We chose anatomical over functional assessment because, were we to intervene, IVUS would have provided us with the morphological details required for successful LMS PCI4 and IVUS over OCT because the latter is often suboptimal for the LMS ostium due to unpredictable and usually poor opacifi cation during pull-back, as the catheter needs to sit outside the anatomical ostium. Tako-Tsubo cardiomyopathy is now well-recognised as a consequence of sudden and excessive catecholamine surges; the list of precipitants includes trauma and is ever-expanding. Recently it has been reported that not only negative but also positive emotions can trigger it5 . We think this is an eloquent illustration of the role of multi-modality imaging in the contemporary assessment of LMS disease as well as of the changing spectrum of ACS presentations.
Conflict of interest: none declared.
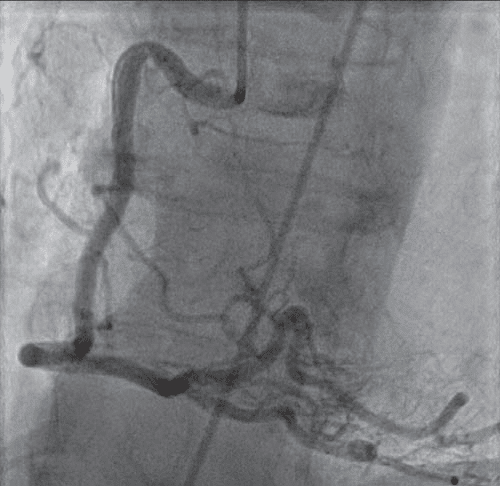
Figure 1. Unobstructed dominant right coronary artery (LAO projection).
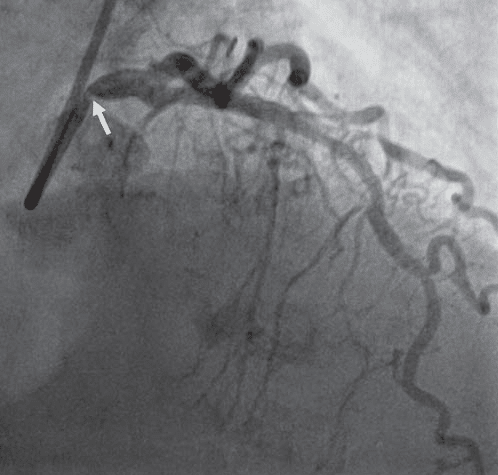
Figure 2. Left coronary arteriogram. Note impression of possibly signifi – cant ostial left main stem (LMS) stenosis (arrow). There was mild pressure damping with a 6F EBU 3.5 guide catheter
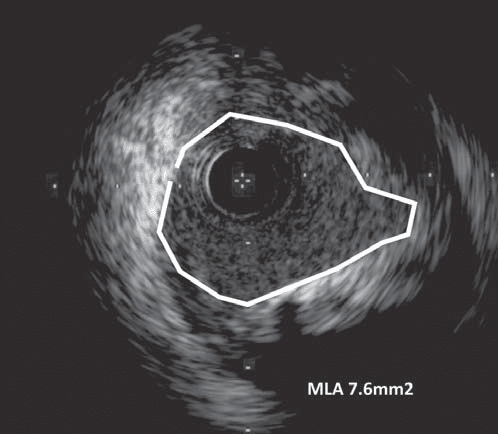
Figure 3. LMS ostium by IVUS. MLA = minimal luminal area.
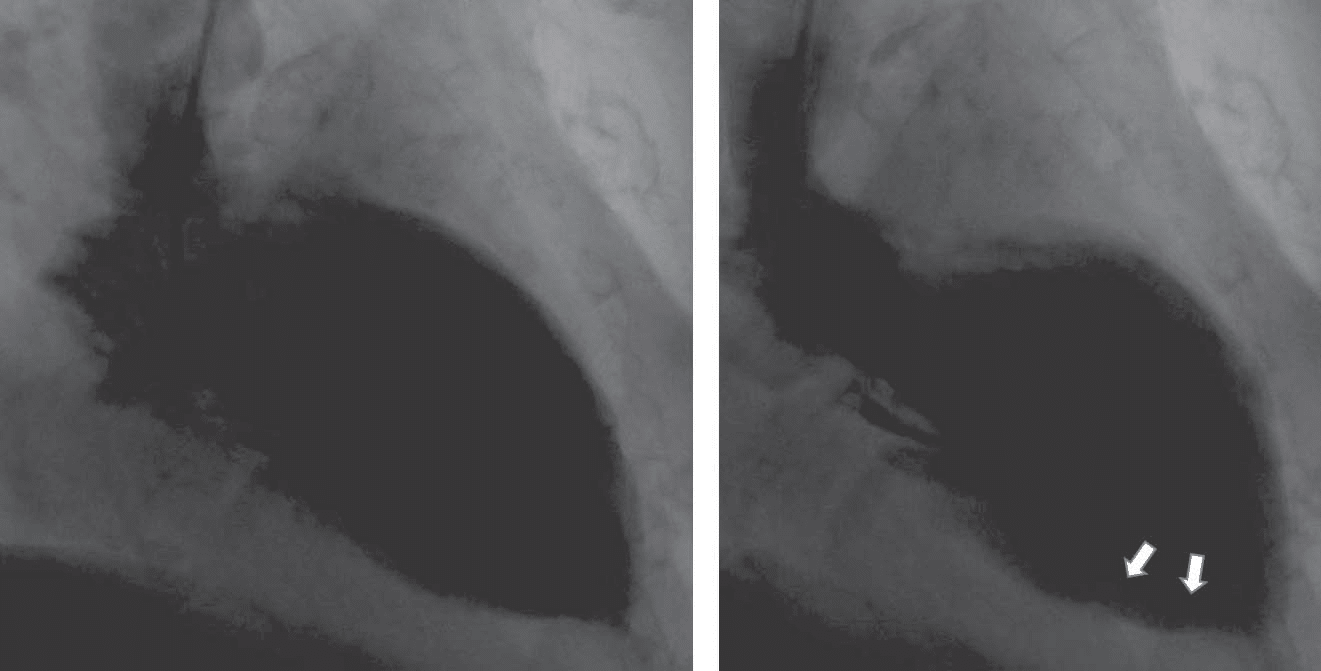
Figure 4. Diastolic (left panel) and systolic (right frame) LV angiography frames. Note typical apical ballooning in systole (arrows).
References
1. Bing R, Yong ASC, Lowe HC. Percutaneous Transcatheter Assessment of the Left Main Coronary Artery: Current Status and Future Directions. J Am Coll Cardiol Intv. 2015;8:1529-1539.
2. Hamilos M, Muller O, Cuisse T et al. Long-Term Clinical Outcome After Fractional Flow Reserve–Guided Treatment in Patients With Angiographically Equivocal Left Main Coronary Artery Stenosis. Circulation. 2009;120:1505-1512.
3. Park SJ, Ahn J-M, S-J Kang et al. Intravascular Ultrasound-Derived Minimal Lumen Area Criteria for Functionally Significant Left Main Coronary Artery Stenosis. J Am Coll Cardiol Intv 2014;7:868–74.
4. Rampat R, Hildick-Smith D. Left Main Stem Percutaneous Coronary Intervention – Data and Ongoing Trials. https://www.radcliffecardiology.com/system/files/articles /ICR%2010.3_132-5.pdf – Accessed on-line 30/10/2016.
5. Ghadri JR, Sarcon A, Diekmann J et al. Happy heart syndrome: role of positive emotional stress in takotsubo syndrome. Accessed on line on 30/10/2016 at doi:10.1093/eurheartj/ehv757.
 This work is licensed under a
This work is licensed under a