Sorin Liviu Bãilã1, Andrei Parnia1, Maria-Magdalena Totir1, Anca Drãgan1, Mihaela Sãlãgean1
1 Emergency Institute for Cadiovascular Diseases “Prof. Dr. C. C. Iliescu” Bucharest, Romania
GENERAL CONSIDERATIONS
Aortic aneurysmal disease affects commonly the ascending aorta and infrarenal aorta. Thoraco-abdominal segment is more rarely affected. The course of the disease is dictated by the risk of rupture. The site of the aneurysm and the visceral branches involved influence the type of surgical repair indicated and the postoperative outcome.
In terms of anatomical disposition, the most common used is Crawford classification1. Type IV Crawford aneurysms are 4% of all thoracoabdominal aneurysms (TAAA). This is the only type of TAAA which is treated by Vascular Surgery specialty1. Surgical treatment of TAAA consists of resecting the aneurysm, reestablish the bloodflow and reimplanting aortic branches when necessary. The outcome is influenced by duration of aortic cross-clamping and by the efficiency of the method used as protection for visceral ischemia2. Possible site of aortic cross-clamping:
- Supradiaphragmatic- risk of paraplegia (Adamkiewicz artery);
- Above the celiac trunk- risk of hepatic, intestinal and renal ischemia;
- Above the renal arteries (and under the superior mesenteric artery) – risk of renal ischemia3,5.
Methods available for protection against visceral ischemia during aortic cross-clamping:
- Reduced clamping time (surgical technique, speed of suture); Continuous perfusion of the visceral branches (renal and intestinal) by a passive shunt from right axillary artery;
- Perfusion of renal arteries by different sollutions (cold Ringer lactate, PgE1, adenosine, manitol, fenoldapam, calcium channel blockers)4.
Retroperitoneal surgical approach allows access of great vessels in the abdomen and their main branches, after rotating the viscera to the left. By extending the incision in the 8th intercostal space and phrenotomy – control is gain of the descending thoracic aorta. Advantages of retroperitoneal approach of the aorta1:
- Less physiologic insult and a smoother postoperative course;
- Less ventilatory support and faster gastrointestinal tolerance recovery;
- It facilitates proximal abdominal aortic exposure and anastomosis, especially in large, pararenal aneurysms or in situations unfavorable to a transabdominal approach; suited to those that pose significant technical challenges. ;
- Adequate exposure to the proximal right renal artery can be obtained.
We present a 52 years old patient with multiple cardiovascular risk factors: arterial hypertension, overweight, dyslipidemia, presenting for intense thoraco-lumbar pain irradiated in the right abdominal flank and groin, aggravated gradually in the last 2 weeks. On admission to the hospital, the patient was anxious with intense abdominal pain; blood pressure was 160/100 mmHg at both arms, heart rate of 105 bpm, regular, the heart was not enlarged, and there were no unusual sounds or murmurs, no signs of systemic or pulmonary stasis. The patient describes weight loss (about 20 kg in the last 3 months), postprandial abdominal angina, abdomen was supple, mobile with breathing, but spontaneously painful and also on palpation in the left upper quadrant, normal intestinal transit, lower limbs with warm skin, distal pulses present.
Laboratory findings revealed dyslipidemia (total cholesterol 278 mg/dl, triglycerides 292 mg/dl), no other abnormal findings.
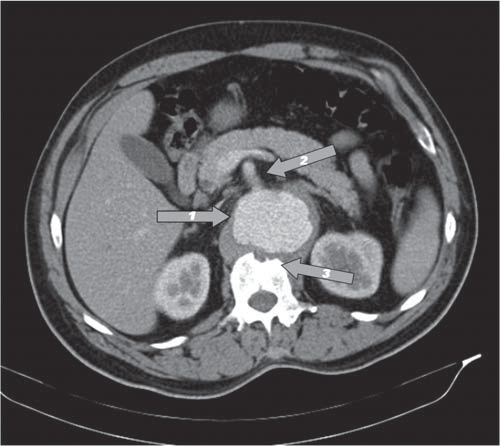
Figure 1.An axial computed tomography (CT) image at the level of the abdominal aorta reveals an visceral aortic aneurysm. 1: Visceral abdominal aortic aneurysm. 2: Superior mesenteric artery origin from the expansion area of the abdominal aortic aneurysm. 3: Erosion of L1 vertebral body adjacent aneurysmal dilation.

Figure 2.CT scan, imaging of a type IV Crawford aortic aneurysm. 1: Visceral aneurysm in the abdominal aorta, partially thrombosed. 2: Celiac trunk origin from the expansion area of the aortic aneurysm.
An electrocardiogram revealed no abnormality.
Transthoracic echocardiography (TTE) was performed and showed important concentric left ventricular hypertrophy (LVH). The septum measured in parasternal long axis was 15 mm and the posterior left ventricular wall 13 mm. The TTE also revealed tricuspid aortic valves with mild ascending aortic dilatation of 40 mm, no signs of dissection of the ascending aorta. The patient has a good wall motion, with a ejection fraction of 50-55%, without significant valvular disease. Diastolic dysfunction was confirmed.
The examination includes a CT scan angiography of chest-abdomen-pelvis which revealed an visceral aortic abdominal sacciform aneurysm of left postero-lateral aorta, 40/35/60 mm size, with mural thrombus. The aneurysm described cause pressure atrophy in the anterior wall of the vertebral body L1. It includes the celiac trunk, superior mesenteric artery and the right renal artery. Its inferior limit is in a horizontal plane immediately cranial to the emergence of left renal artery. There were detected significant soft and calcified plaque that interest aorta and its most important branches. Thoracic aorta has tortuous course, with the following diameters: 40 mm of ascending aorta, aortic arch – 30 mm, descending aorta (at the level of pulmonary artery) – 27 mm, distal descending aorta (at the level of a plane passing through T10) – 41 mm, dilated.
Conclusions of CT scan angiography: Abdominal aortic sacciform aneurysm, with the involvement of emerging of celiac trunk, superior mesenteric artery and right renal artery (Figure 2) – compatible with type IV Crawford TAAA.
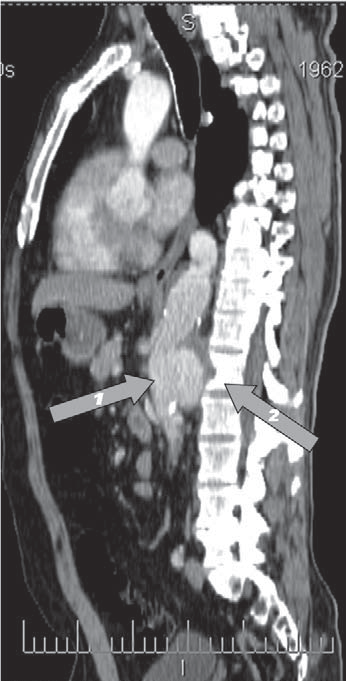
Figure 3. CT scan, imaging of a type IV Crawford aortic aneurysm. 1: Abdominal aortic aneurysm. 2: Erosion of L1 vertebral body adjacent aneurysmal dilation.
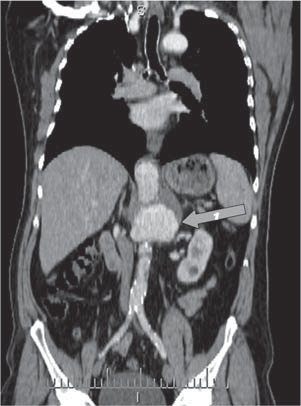
Figure 4. CT scan of partially thrombosed aneurysm in visceral abdominal aorta.
Because of symptomatic aneurysm, surgery was decided. Open surgical repair of type IV Crawford TAAA was performed through a mixt exposure of the aorta – retroperitoneal and thoracic with phrenotomy – with the patient under general endotracheal anesthesia (Figure 5).
Figure 5. Canulas for nepfoplegia.
Intraoperative – saciform visceral abdominal aorta aneurysm with a maximum diameter of 5 cm was found, developed left posterolateral, that erodes L1 ver-ebral body. The aneurysm included all the abdominal aortic visceral branches, excepting left renal artery. Supraceliac aortic cross-clamping was performed, and of all means available, we used cold nephroplegia with Alprostadil (retrograde renal artery perfusion with cold heparinated Ringer solution with Alprostadil (PgE1) (Figure 5). It was practiced aortic aneurismectomy and visceral abdominal aorta angioplasty with Dacron patch (Figure 6).
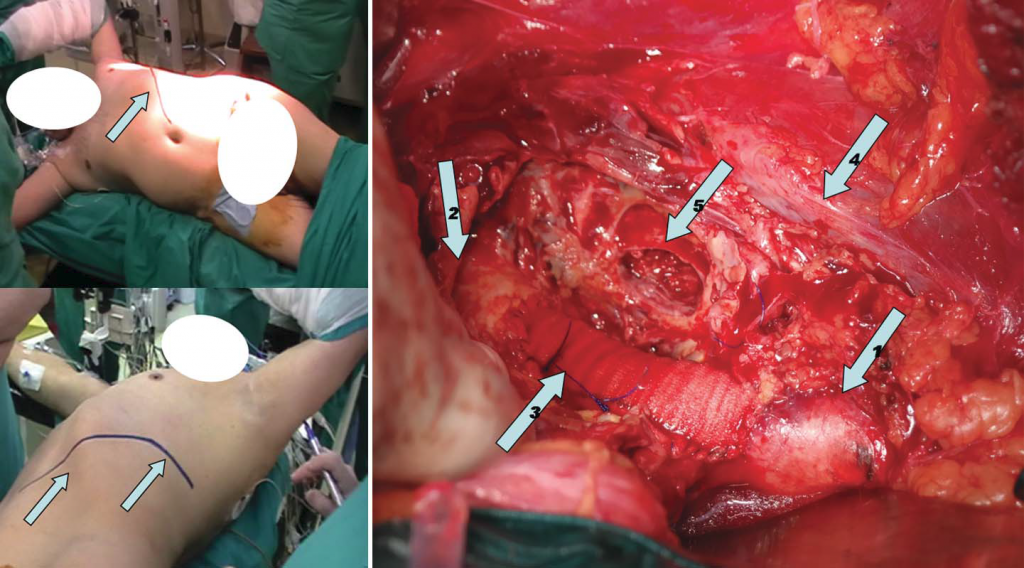
Figure 6. (Left image) Patient position for mixt approach- abdominal (retroperitoneal) and thoracic. Arrows: Incision line for thoracophrenolaparotomy (Right image) Open repair of type IV Crawford TAAA- fi nal aspect. 1: Supraaneurysmal visceral aorta. 2: Infraaneurysmal visceral aorta. 3: The angioplasty Dacron patch. 4: Inferior vena cava. 5: Erosion area in the L1 vertebral body.
The postoperative evolution of the patient was favorable without local or systemic complications. Conflict of interest: none declared.
References
1. Edward Y. Woo, Scott M. Damrauer. Abdominal Aortic Aneurysms: Open Surgical Treatment. In: Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery, editors. 8th ed. Philadelphia: WB Saunders
Co; 2014. pp 2024-2046.
2. Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, Evangelista A, Falk V, Frank H, Gaemperli O, Grabenwöger M, Haverich A, Iung B, Manolis AJ, Meijboom F, Nienaber CA, Roffi
M, Rousseau H, Sechtem U, Sirnes PA, Allmen RS, Vrints CJ. ESC Committee for Practice Guidelines (CPG). 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering
acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Th e Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 2014 Nov;35(41):2873–2926.
3. Sandmann W, Grabitz K, Kniemeyer HW, Stühmeier K, Breulmann M. Chirurgische Behandlung des thorako- abdominalen und suprarenalen Aortenaneurysmas. Zentralbl Chir.1988;113(20):1305–1314.
4. Torsello G, Kutkuhn B, Kniemeyer H, Sandmann W: Prevention of acute renal failure in suprarenal aortic surgery. Results of a pilot study. Zentralbl Chir 118(7): 390 -394, 1993.
5. Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Th oracoabdominal aortic aneurysms associated with celiac, superior mesenteric, and renal artery occlusive disease: methods and analysis of results in 271 patients. J Vasc Surg 1992;16:378–389.
 This work is licensed under a
This work is licensed under a