Anca D. Mateescu1,2, Roxana Enache1,2, Andreea Calin1,2, Dan Deleanu2, Carmen Ginghina1,2, Bogdan A. Popescu1,2
1 „Carol Davila” University of Medicine and Pharmacy, Euroecolab, Bucharest
2 „Prof. Dr. C. C.Iliescu” Emergency Institute for Cardiovascular Diseases, Bucharest
Contact address:
Bogdan A. Popescu
“Carol Davila” University of Medicine and Pharmacy, Euroecolab,
“Prof. Dr. C. C. Iliescu” Emergency Institute for Cardiovascular Diseases
258 Fundeni Avenue, 2nd District, 022328, Bucharest, Romania, Phone/Fax: +40213175227. E-mail: bogdan.a.popescu@gmail.com
Anomalies of origin and distribution of the coronary arteries are unusual malformations1. They may occur in multiple forms and may produce striking physical findings and sometimes serious cardiac disability. Anomalous single coronary artery with coronary fistula is a rare finding2. Coronary artery fistula (CAF) is most often diagnosed by echocardiography or coronary angiography and there is a higher incidence of CAF to right heart chambers, while CAF to the left ventricle is rare3.
A 42-year-old woman was referred for cardiac evaluation for non-specific chest pain over the past 8 months. Physical examination revealed a systolic thrill at the left sternal border and a loud systolic and diastolic murmur over the entire precordium. The diastolic component was rather high pitched. The blood pressure was 100/70 mm Hg and the peripheral pulses were normal. There were no additional abnormalities on physical examination. The ECG showed sinus rhythm at 65 bpm and incomplete right bundle branch block. Transthoracic and transesophageal echocardiography revealed an unusual echo free circular structure (1.8/2.2 cm in size), located in the right ventricle just beneath the tricuspid valve (Figure 1), with an abnormal turbulent flow at color Doppler examination (Figure 2). A continuous systolic-diastolic flow signal with high velocities (up to 4 m/s) was recorded by continuous wave Doppler examination at the level of this turbulent jet (Figure 3). Mild to moderate aortic regurgitation due to mild dilatation of the aortic root was also noted. Both left ventricular volumes and systolic function were normal, with no wall motion abnormalities. Coronary angiography showed an unusual single coronary artery arising from the left coronary sinus and terminating into the right ventricle through a coronary-cavity fistula (Figure 4). The left anterior descending, the circumflex and the right coronary arteries were all arising from the single vessel. On cardiac catheterization, all the intracardiac and intravascular pressures were normal, with no intracardiac shunt. Considering the atypical chest pain, the normal left ventricular volumes and function and the absence of a left-to-right shunt, surgery was not recommended.
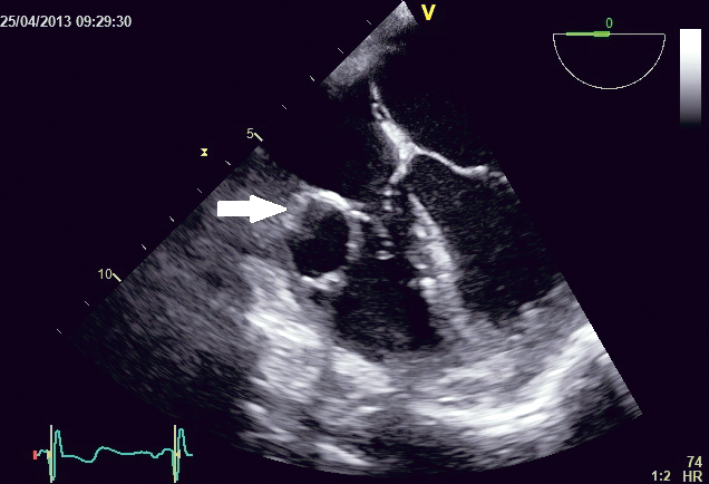
Figure 1. TEE examination, 4 chamber view; an echo free circular structure (1.8/2.2 cm in size) can be seen in the right ventricle, just beneath the tricuspid valve (arrow).
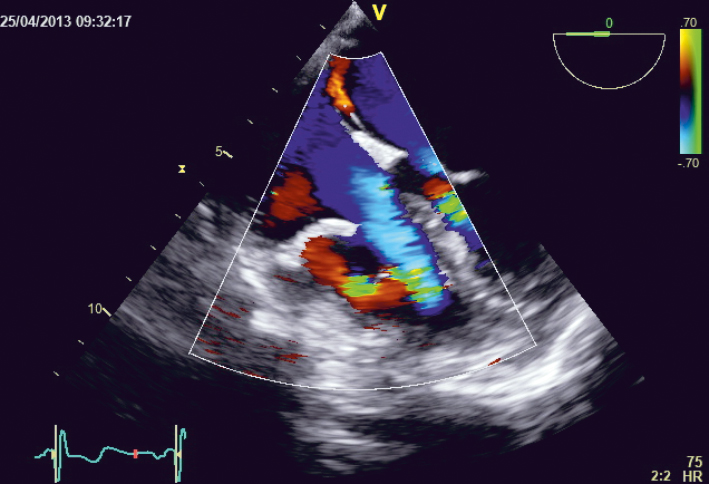
Figure 2. TEE examination, 4 chamber view; TEE reveals an abnormal turbulent flow at color Doppler examination at the level of this circular structure located in the right ventricle.
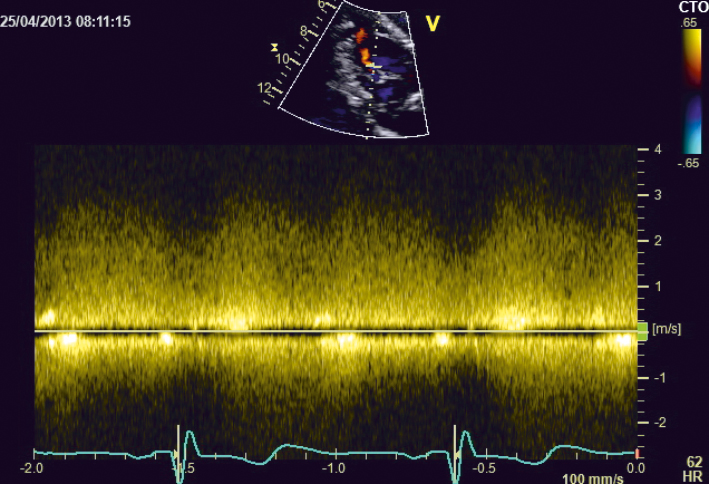
Figure 3. TTE examination, modified 4 chamber view; A continuous systolic-diastolic flow signal with high velocities (up to 4 m/s) was recorded by CW Doppler at the level of the turbulent jet.

Figure 4. Coronary angiogram, aortic root injection, left anterior oblique caudal projection. A single coronary artery is seen arising from the left coronary sinus and terminating into the right ventricle through a coronary-cavity fistula. The dilatation of this single coronary artery can be easily appreciated.
The role of transthoracic and transesophageal echocardiography in the diagnosis of coronary fistulas is well recognized. Cardiac catheterization is a very useful diagnostic test, not only to evaluate the hemodynamic status but also to diagnose the presence of a single coronary artery1,4.
Conflict of interest: none declared.
References
1. Phasalkar M, Thakkar B, Poptani V. Successful transcatheter closure of coronary artery fistula in a child with single coronary artery: a heavy
load and a long road. Catheter Cardiovasc Interv. 2013; 82(1):150-4.
2. Murray RH: Single coronary artery with fistulous communication. Circulation 1963; 28:437.
3. Gupta PD, Rahimtoola SH, Miller RA. Single coronary artery-right ventricle fistula. British Heart Journal 1972; 34:755-757.
4. Imbalzano E, Dattilo G, Scarpelli M, Lo Gullo A, Saitta A. Left coronary artery fistula to right ventricle complicated heart failure in a patient on hemodialysis. Journal Internal and Emergency Medicine 2013; 8:765.
 This work is licensed under a
This work is licensed under a